WebRTC has revolutionized real-time communication for healthcare applications, from telemedicine consultations to remote patient monitoring. However, enterprise healthcare networks present unique challenges that can render even the most sophisticated WebRTC implementations ineffective. Understanding these constraints and designing resilient solutions is critical for delivering reliable healthcare communication systems.
The Promise and Reality of WebRTC in Healthcare
WebRTC enables peer-to-peer audio, video, and data transmission directly between browsers without plugins or additional software. This technology seems perfect for healthcare: doctors can connect with patients instantly, specialists can collaborate in real-time, and medical devices can stream vital signs directly to clinicians.
The reality, however, is more complex. Hospital networks operate under security constraints that would seem draconian in most industries. A telemedicine platform that works flawlessly on consumer networks may completely fail when a doctor attempts to connect from within a hospital’s secure environment. Research from healthcare IT implementations shows that doctors in many hospital networks can only access port 80 through their firewall when connecting to external systems. This restriction alone breaks most standard WebRTC configurations.
Understanding Enterprise Network Constraints
The Firewall Fortress
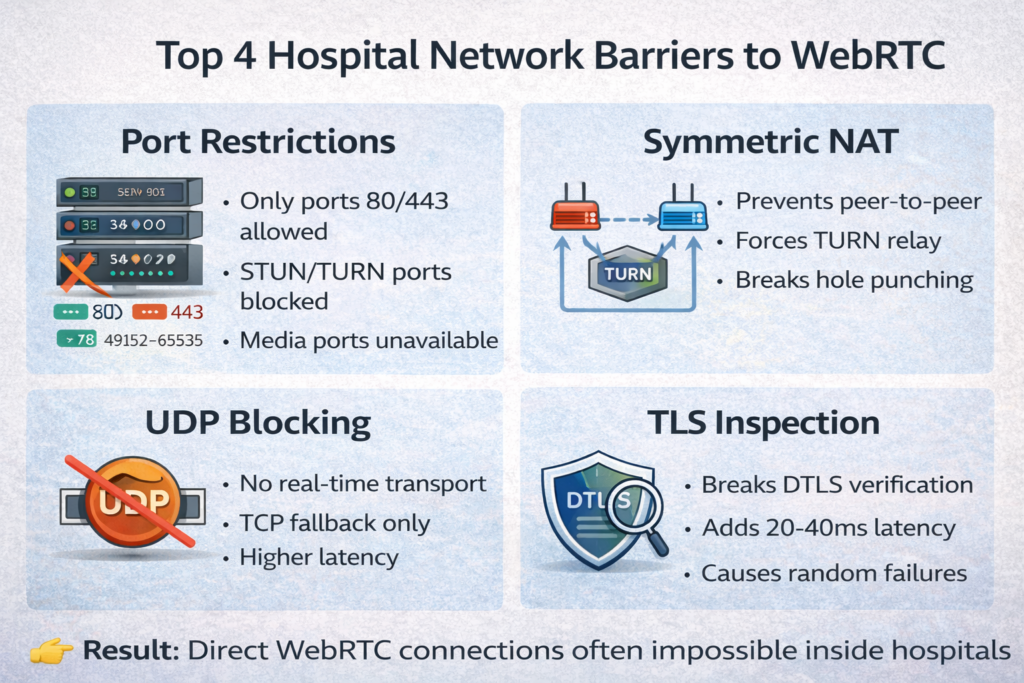
Hospital networks implement multiple layers of security to protect patient data and comply with regulations like HIPAA. These protections create significant barriers for WebRTC traffic:
Restrictive Port Policies: Unlike consumer networks that typically allow a wide range of ports, hospital firewalls often whitelist only essential ports. Standard WebRTC implementations require access to:
- UDP ports 3478 (STUN/TURN)
- UDP ports 49152-65535 (WebRTC media)
- TCP port 443 (HTTPS)
When only ports 80 and 443 are available, traditional WebRTC connection establishment fails entirely.
Symmetric NAT: Many enterprise networks deploy symmetric NAT configurations, which assign different external ports for each unique destination. This breaks the hole-punching techniques that WebRTC typically relies on for peer-to-peer connections. Even with STUN servers, symmetric NAT prevents direct peer connections, forcing all traffic through relay servers.
Protocol Blocking: Some hospital networks block UDP traffic entirely at the application layer, regardless of port. Since WebRTC relies heavily on UDP for low-latency media transmission, this creates an immediate compatibility problem.
TLS Inspection: The Silent Killer
Transport Layer Security inspection has become ubiquitous in enterprise networks, and healthcare is no exception. While TLS inspection serves legitimate security purposes, it introduces complications for WebRTC:
Certificate Chain Disruption: TLS inspection works by intercepting encrypted traffic, decrypting it with a wildcard certificate, inspecting the content, and re-encrypting it before forwarding. For WebRTC, which relies on DTLS certificates for peer verification, this process can break certificate fingerprint validation.
Latency Introduction: The decrypt-inspect-encrypt cycle adds processing overhead. While this may be negligible for web browsing, real-time communication is sensitive to even small latency increases. Research indicates that each inspection layer can add 18-20 milliseconds of latency, which accumulates across multiple concurrent streams.
Deep Packet Inspection: Some enterprise firewalls employ deep packet inspection that throttles or blocks traffic patterns associated with WebRTC, even when the traffic uses approved ports. This creates unpredictable connectivity issues that are difficult to diagnose.
| Network Constraint | Impact on WebRTC | Prevalence in Healthcare |
| Port restrictions | Blocks STUN/TURN and media ports | Very High (80-90%) |
| Symmetric NAT | Prevents peer-to-peer connections | High (60-70%) |
| UDP blocking | Forces TCP fallback, increases latency | Medium (30-40%) |
| TLS inspection | Breaks DTLS verification, adds latency | High (70-80%) |
| Protocol filtering | Unpredictable connection failures | Medium (40-50%) |
TURN Server Overload: The Scalability Trap
When peer-to-peer connections fail, WebRTC falls back to TURN (Traversal Using Relays around NAT) servers, which relay all media traffic. This fallback mechanism, while essential for reliability, introduces its own set of challenges.
The Resource Consumption Problem
TURN servers must relay every packet of audio and video data, consuming significant bandwidth and processing resources. A single HD video call can require 3-5 Mbps of bandwidth in each direction. When dozens or hundreds of healthcare workers simultaneously use telemedicine systems, the TURN server capacity becomes the bottleneck.
Consider a hospital network where 50 doctors conduct video consultations simultaneously. If restrictive firewall policies force all connections through TURN servers, the infrastructure must handle:
- 150-250 Mbps of aggregate bandwidth
- Thousands of packets per second require processing and forwarding
- Stateful session management for all active connections
Cost and Infrastructure Implications
TURN infrastructure is expensive to scale. Unlike stateless services that can distribute load easily, TURN servers maintain session state for each active connection. This means:
Vertical Scaling Limitations: Adding more CPU and memory to existing TURN servers helps, but eventually hits physical hardware limits. A server that handles 100 concurrent sessions might need quadruple the resources to handle 200 sessions due to overhead.
Horizontal Scaling Complexity: Distributing TURN load across multiple servers requires sophisticated load balancing that accounts for geographic distribution, session affinity, and network topology. Simply adding more servers doesn’t automatically distribute the load.
Geographic Distribution: For global healthcare networks, TURN servers must be geographically distributed to minimize latency. This multiplies infrastructure costs and management complexity.
The Hidden Costs
Beyond direct infrastructure costs, TURN relays introduce:
- Increased latency (typically 50-200ms additional round-trip time)
- Reduced video quality due to bandwidth constraints
- Single points of failure that can disrupt hundreds of calls
- Complex capacity planning and monitoring requirements
Designing Resilient Solutions
Successfully deploying WebRTC in healthcare environments requires anticipating these constraints and building robust fallback mechanisms. Here are proven architectural patterns:
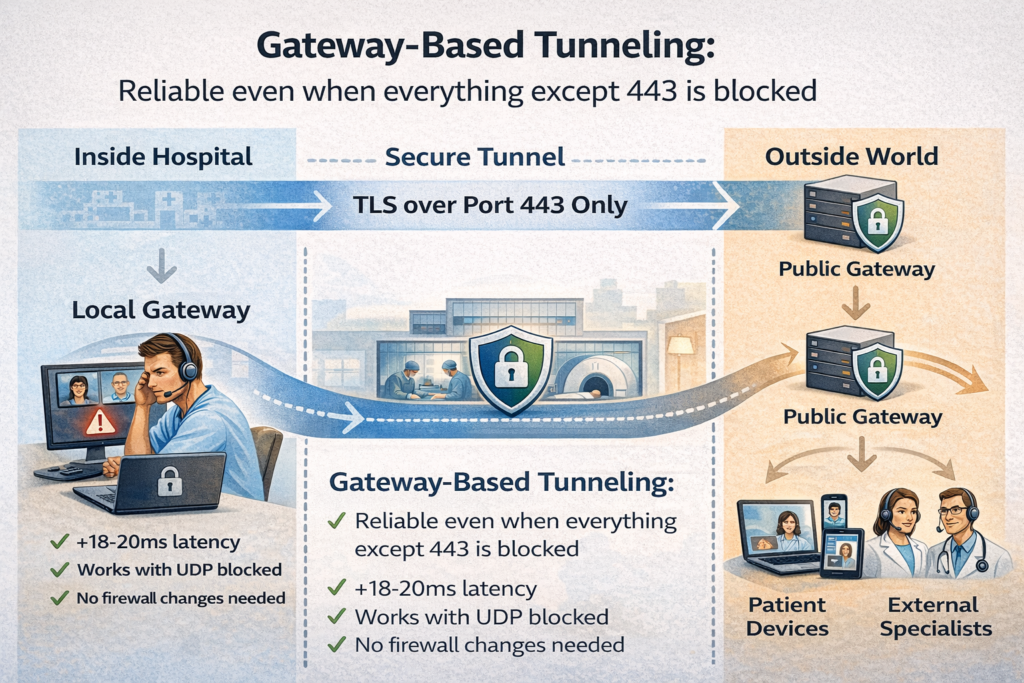
1. Gateway-Based Tunneling
Instead of relying on individual client devices to navigate firewall restrictions, implement local gateway services within the hospital network. This architecture works by:
Local Gateway Deployment: Install a gateway service inside the hospital network that handles all WebRTC traffic. Hospital-based clients connect to this local gateway using unrestricted internal network ports.
Secure Tunnel Establishment: The local gateway maintains a persistent, secure tunnel to an external public gateway using only port 443 with TLS. This tunnel can carry multiple concurrent WebRTC sessions.
Traffic Routing: The public gateway routes media streams between hospital gateways and external clients (patients at home, specialists at other facilities) without requiring complex firewall configurations.
This approach has demonstrated success in healthcare deployments, adding only 18-20 milliseconds of latency per stream while completely bypassing firewall restrictions.
2. Adaptive Transport Selection
Implement intelligent transport selection that probes network conditions and selects the optimal connection method:
Priority 1: Direct UDP peer connection (lowest latency, best quality)
Priority 2: TURN over UDP (moderate latency, reliable)
Priority 3: TURN over TCP (higher latency, firewall-friendly)
Priority 4: TURN over TLS on port 443 (highest compatibility)
Priority 5: WebSocket fallback for signaling and low-bandwidth data
The system should attempt each method in sequence, falling back only when necessary. For environments where UDP is completely blocked, configuring TURN servers to support TCP and TLS on port 443 ensures connectivity.
3. Hybrid Signaling Architecture
Separate the signaling path from the media path, using different protocols optimized for each:
Signaling: Use secure WebSockets (WSS) over port 443 for all signaling traffic. This ensures firewall compatibility and enables load balancing across multiple signaling servers.
Media: Attempt direct WebRTC connections first, but maintain the ability to fall back to HTTP-based transports if necessary. For extremely restrictive environments, consider chunked transfer encoding over HTTPS as a last resort.
Data Channels: For non-real-time data (chat messages, file transfers, clinical notes), use WebSocket as the primary transport rather than WebRTC data channels. This reduces TURN server load and improves reliability.
4. Intelligent TURN Infrastructure
Design TURN infrastructure for enterprise scale:
Dynamic Port Allocation: Configure TURN servers to operate on standard ports (443, 3478) but implement dynamic port allocation within allowed ranges to reduce port exhaustion.
Geographic Load Balancing: Deploy TURN servers in multiple regions and use DNS-based load balancing to direct clients to the nearest server. Monitor session distribution and automatically adjust routing to prevent overload.
Session Affinity: Ensure that all media streams for a single call use the same TURN server to minimize latency and packet reordering.
Monitoring and Auto-scaling: Implement real-time monitoring of TURN server metrics (CPU usage, bandwidth consumption, active sessions) and automatically provision additional capacity when thresholds are exceeded.
5. Certificate Management for TLS Inspection
Work proactively with hospital IT security teams to whitelist your WebRTC application from TLS inspection:
Documented Security Posture: Provide comprehensive security documentation showing that WebRTC uses end-to-end encryption (DTLS/SRTP) that makes TLS inspection redundant.
Compliance Evidence: Demonstrate HIPAA compliance through encryption methods, access controls, and audit logging built into your application.
Bypass Configuration: Help IT teams configure their TLS inspection devices to exclude your application’s domains, preserving DTLS certificate verification while maintaining their security policies.
Testing and Validation
Rigorous testing in representative environments is essential. Create a testing strategy that includes:
Network Simulation
Build test environments that replicate hospital network constraints:
- Configure firewalls to allow only ports 80 and 443
- Implement symmetric NAT
- Block UDP traffic entirely in some test scenarios
- Add TLS inspection proxies that break certificate chains
- Introduce artificial latency (50-150ms) to simulate WAN links
Load Testing
Validate TURN infrastructure under realistic load:
- Simulate 100+ concurrent sessions through TURN servers
- Measure bandwidth consumption, CPU usage, and latency
- Identify breaking points and capacity limits
- Test failover scenarios when TURN servers go offline
User Acceptance Testing
Conduct trials with actual healthcare providers in production networks:
- Deploy in pilot hospital departments before full rollout
- Collect feedback on connection reliability and quality
- Monitor real-world success rates for different connection types
- Measure user satisfaction and identify pain points
Partnering for Success
Implementing WebRTC in healthcare environments requires specialized expertise in network architecture, real-time communications, and healthcare IT security. The challenges are technical, but they’re also organizational—success requires collaboration between development teams, hospital IT departments, and security professionals.
This is where partnering with an experienced technology provider becomes invaluable. Trembit brings deep expertise in building resilient WebRTC solutions for complex enterprise environments. Our team understands the unique constraints of healthcare networks and has successfully navigated firewall restrictions, TLS inspection, and scalability challenges across multiple healthcare deployments.
We work collaboratively with your IT security teams to design solutions that meet both functional requirements and security policies. From gateway architecture design to TURN infrastructure optimization, Trembit provides the technical depth and healthcare industry knowledge needed to deliver reliable telemedicine and communication platforms.
Looking Forward
As healthcare continues its digital transformation, reliable real-time communication becomes increasingly critical. The network constraints that break standard WebRTC implementations aren’t going away — if anything, security requirements will become more stringent.
Success requires understanding these constraints, designing with resilience from the start, and partnering with experts who have solved these problems before. The technical challenges are significant, but they’re surmountable with the right architecture, testing methodology, and implementation expertise.
By anticipating network restrictions, building adaptive fallback mechanisms, and designing scalable infrastructure, you can deliver WebRTC solutions that work reliably in even the most restrictive healthcare environments. The result is better patient care through improved clinical communication, no matter what network constraints stand in the way.
About the Author: This article was created to help healthcare technology teams understand and overcome the unique challenges of implementing WebRTC in enterprise hospital networks. For more insights on healthcare technology solutions, visit trembit.com.
Ready to build a resilient telemedicine platform? Trembit’s experienced team can help you navigate the complexities of WebRTC in healthcare environments. Contact us to discuss your project requirements and learn how we can help deliver reliable real-time communication solutions for your healthcare organization.