The promise of telemedicine is simple: deliver healthcare anywhere, at any time, with the same quality as an in-person visit. However, achieving this promise creates a fundamental tension between two critical requirements — HIPAA compliance and video performance. Healthcare organizations must simultaneously protect patient privacy through rigorous security measures while delivering the low-latency, high-quality video experience that clinical care demands.
This conflict is not theoretical. Every encryption layer, every audit log entry, and every compliance mechanism adds overhead that can degrade the real-time communication experience. Understanding how to balance these competing demands is essential for building telemedicine platforms that are both legally compliant and clinically effective.
The Dual Mandate: Security and Speed
WebRTC was designed with security in mind. The protocol mandates encryption through DTLS-SRTP, protecting media streams from interception. For most consumer applications, this built-in security is sufficient. Healthcare, however, operates under a different set of standards entirely.
HIPAA compliance necessitates multiple layers of protection that extend beyond what WebRTC provides natively. Organizations must implement end-to-end encryption that survives media server routing, comprehensive audit logging of every access to protected health information, secure key management and rotation, authenticated access controls with multi-factor authentication, and encrypted storage for session recordings. Each of these requirements introduces latency, processing overhead, or both.

Consider the journey of a single video frame in a HIPAA-compliant telemedicine session. The frame is captured by the camera, encoded using a video codec (typically VP8 or H.264), encrypted by WebRTC’s SRTP layer, potentially re-encrypted with an additional end-to-end encryption layer, transmitted across the network through firewalls and TURN servers, logged for audit purposes at multiple checkpoints, decrypted and re-encrypted by media servers if routing is required, and finally decrypted and rendered on the receiving device. Every step adds microseconds to milliseconds of delay. When you’re targeting the sub-500ms latency that makes conversation feel natural, those delays accumulate quickly.
Encryption Layers: The Performance Tax
WebRTC’s native encryption using DTLS-SRTP provides hop-to-hop security, meaning data is encrypted during transmission but decrypted at intermediary servers like Selective Forwarding Units (SFUs) that route media in multi-party calls. For consumer applications, this is acceptable—the SFU operator is trusted. For HIPAA compliance, however, trusting the infrastructure provider is not sufficient. Regulations require protection against unauthorized access, which includes scenarios where the infrastructure itself might be compromised.
The solution is additional end-to-end encryption that keeps media encrypted even at the media server level. This approach ensures that only authorized participants, the doctor and patient, can decrypt the video and audio streams, not the servers routing them. While essential for compliance, this additional encryption layer creates measurable performance impacts.
Modern end-to-end encryption implementations for WebRTC use frame-level encryption, where each video and audio frame is encrypted individually before being passed to WebRTC’s SRTP layer. This approach provides several advantages: it operates on complete frames rather than individual packets, reducing overhead; it maintains compatibility with existing SFU infrastructure; and it enables selective encryption where non-sensitive metadata remains accessible for routing decisions.
However, the computational cost is significant. Encryption operations for each frame require CPU cycles that could otherwise be used for video encoding or other application logic. Research into frame-level encryption overhead shows that the additional processing can consume 5-15% more CPU resources depending on the encryption algorithm and key size used. For mobile devices with limited processing power, this overhead can force a reduction in video quality or frame rate to maintain acceptable battery life.
The impact varies by implementation approach. Using web workers to offload encryption from the main JavaScript thread can mitigate UI performance issues, but doesn’t eliminate the underlying computational cost. Hardware-accelerated encryption, where available, can significantly reduce the overhead — but not all devices support hardware acceleration for the specific encryption algorithms used in WebRTC frame encryption.
Encryption Architecture Decisions
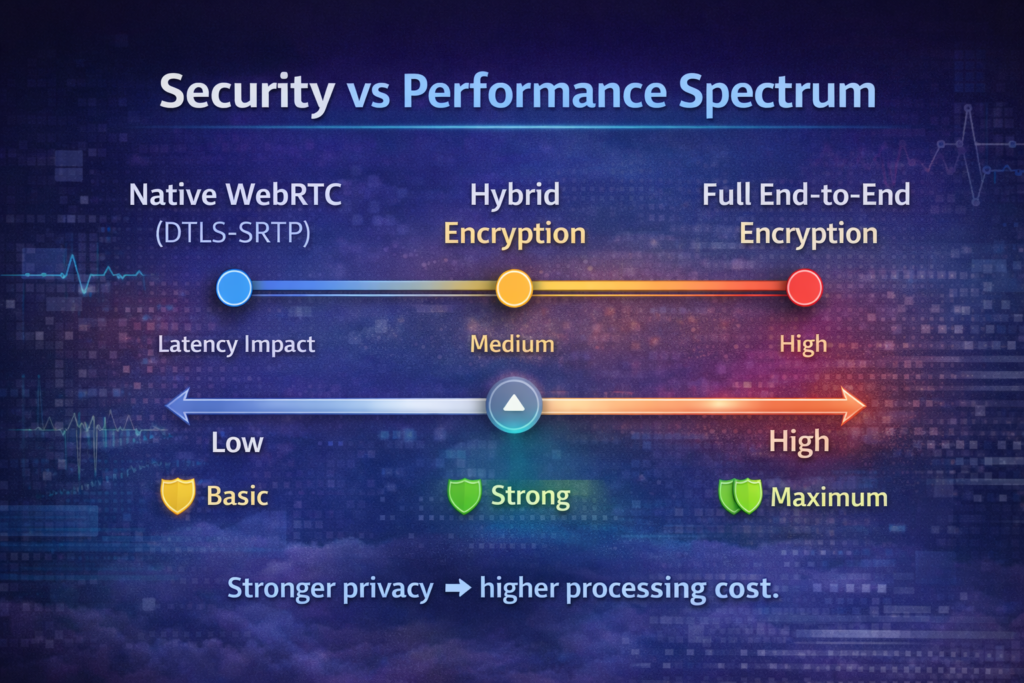
Healthcare organizations must choose between several encryption architecture patterns, each with distinct performance characteristics:
Standard WebRTC with Enhanced SFU Security: Use WebRTC’s native DTLS-SRTP encryption and deploy media servers within a HIPAA-compliant hosting environment with strict access controls. This approach minimizes performance overhead but requires absolute trust in the infrastructure provider and comprehensive Business Associate Agreements covering every vendor with access to unencrypted media.
Hybrid Encryption with Selective Protection: Apply end-to-end encryption only to video and audio containing visible or audible PHI, while allowing non-sensitive communication (screen sharing of de-identified data, for example) to use standard encryption. This reduces computational overhead but requires careful classification of data streams and introduces complexity in managing multiple encryption modes within a single session.
Full End-to-End Encryption: Encrypt all media end-to-end regardless of content. This maximizes security and simplifies compliance but carries the highest performance cost. Organizations choosing this approach must carefully manage client-side performance, implement efficient key management, and potentially accept quality reductions on lower-powered devices.
| Encryption Approach | Latency Impact | CPU Overhead | Compliance Strength | Implementation Complexity |
| Standard DTLS-SRTP only | Baseline | Baseline | Requires trusted infrastructure | Low |
| DTLS-SRTP + SFU-level encryption | +10-30ms | +5-10% | Good with proper BAAs | Medium |
| Frame-level E2EE (worker-based) | +20-50ms | +10-20% | Excellent | High |
| Frame-level E2EE (main thread) | +30-80ms | +15-30% | Excellent | High |
| Hardware-accelerated E2EE | +5-15ms | +2-5% | Excellent | Very High |
These numbers represent typical impacts in production environments. Actual results depend on factors including client device capabilities, network conditions, video resolution and frame rate, number of participants in the session, and efficiency of the encryption implementation.
Recording Strategies: Compliance Versus Performance
HIPAA requires documentation of telemedicine encounters, which often means recording video consultations. However, recording encrypted media streams introduces unique challenges. If recordings are captured at the media server level — the most straightforward approach — the media must be decrypted for recording and then re-encrypted for storage. This decrypt-record-encrypt cycle creates several problems.
First, it increases the server’s computational burden. Media servers must now decrypt streams, write uncompressed video to disk or memory, compress and encrypt the recording, all while continuing to route live media to participants. This can double or triple the CPU and memory requirements per active session. Second, it creates a brief window where unencrypted PHI exists in server memory, increasing the attack surface. Third, it complicates key management, as the recording must be encrypted with keys that allow authorized retrieval later while preventing unauthorized access.
The alternative is client-side recording, where one participant’s device (typically the provider’s) records the encrypted media stream locally. This approach eliminates server-side overhead and ensures the media server never accesses unencrypted PHI. However, it introduces its own challenges. Client-side recording adds significant load to the recording device’s CPU and storage, potentially degrading video quality during the consultation itself. Network interruptions on the recording device can cause partial or failed recordings. Synchronizing multiple streams (video, audio, screen sharing) becomes the client’s responsibility.
Organizations must also consider recording format and quality. High-quality recordings suitable for clinical review require higher bitrates and resolution, increasing both bandwidth consumption and storage requirements. A 30-minute HD video consultation can generate 1-2GB of recorded data, which must be encrypted, transferred to secure storage, indexed for retrieval, and retained for HIPAA’s required six-year minimum retention period.
Recording Architecture Patterns
Several architectural approaches have emerged for managing recordings in HIPAA-compliant telemedicine platforms:
- Distributed Recording with Server Aggregation: Participants record locally in encrypted format, then securely upload recordings to central storage after the session. The server aggregates multiple recordings for quality assurance and creates a single authoritative record.
- Selective Recording Trigger: Record only sessions that meet specific criteria (first visits, specific diagnoses, quality assurance samples) rather than recording everything. This reduces storage and processing overhead while maintaining compliance for documented encounters.
- Ephemeral Decryption Service: Deploy a dedicated, isolated service that temporarily decrypts media solely for recording purposes, operates in a hardened environment with extensive audit logging, and destroys decrypted data immediately after recording completes.
- Progressive Enhancement Recording: Start with an audio-only recording (minimal overhead), add low-resolution video snapshots at intervals, and capture a full HD recording only when clinically necessary or when triggered by the provider.
Each approach balances performance, security, and usability differently. The optimal choice depends on organizational risk tolerance, technical capabilities, and clinical workflow requirements.

Audit Logging: The Hidden Performance Killer
HIPAA’s audit control requirement mandates that organizations record and examine activity in systems containing ePHI. For telemedicine platforms, this means logging every session establishment, every participant join and leave event, every change in video or audio settings, every frame of video transmitted (at minimum, metadata about it), and every access to recorded sessions.
The performance impact of comprehensive audit logging is often underestimated. Writing audit log entries is an I/O operation that can create contention with media streaming, especially on systems where disk I/O is a bottleneck. Each log write introduces latency, typically 1-5 milliseconds for writing to local storage or 10-50 milliseconds for writing to remote log aggregation services. While these numbers seem small, they accumulate rapidly in high-throughput scenarios.
Consider a telemedicine platform handling 100 concurrent video sessions. With comprehensive audit logging capturing events at the granularity HIPAA requires, the system might generate several thousand log entries per second. If each log write takes 5ms and blocks the logging thread, the system quickly becomes CPU-bound on logging operations alone.
The challenge intensifies when logs must be written to tamper-evident storage. HIPAA-compliant audit logs must be immutable—once written, they cannot be altered or deleted without detection. Implementing immutability typically requires cryptographic hash chains, where each log entry contains a hash of the previous entry, creating a verifiable sequence. Computing these hashes adds computational overhead to every log write.
Optimizing Audit Performance
Several strategies can mitigate the performance impact of audit logging:
- Asynchronous Logging: Decouple log generation from log persistence by writing logs to an in-memory queue first, then asynchronously flushing to persistent storage. This prevents I/O operations from blocking real-time media operations. However, asynchronous logging introduces the risk of log loss if the system crashes before the queue is flushed.
- Batched Log Writes: Aggregate multiple log entries and write them as a single batch operation. This reduces the number of I/O operations and improves throughput. The tradeoff is increased latency between event occurrence and log persistence, which may be problematic for real-time security monitoring.
- Tiered Logging Architecture: Write critical security events (authentication, authorization, access to PHI) to high-reliability, low-latency storage immediately. Write operational events (session metrics, quality statistics) to a separate, higher-latency system that can tolerate more overhead. This ensures critical compliance data is captured reliably while reducing overall system load.
- Structured Logging with Compression: Use structured log formats (JSON, Protocol Buffers) that compress efficiently and can be indexed quickly. This reduces storage requirements and improves query performance when logs must be retrieved for audit review or incident investigation.
- Dedicated Logging Infrastructure: Separate logging infrastructure from media processing infrastructure entirely. Use dedicated log aggregation services (SIEM platforms, managed logging services) that are optimized for high-volume log ingestion and long-term retention. This prevents logging operations from competing with media processing for system resources.
Organizations implementing these optimizations must carefully balance performance gains against compliance requirements. For example, asynchronous logging with a 10-second flush interval might be acceptable for operational logs but unacceptable for authentication events where immediate persistence is critical for security.
Real-World Performance Scenarios
Understanding the theoretical impacts of compliance measures is important, but practical implementation reveals how these factors combine in production environments. Let’s examine several real-world scenarios:
Scenario 1: Primary Care Video Visit
- One provider, one patient
- 20-minute consultation with screen sharing for lab results
- Standard HD video (720p, 30fps)
- Recording required for medical records
Without compliance overhead, this session would consume approximately 40-50 Mbps of total bandwidth (bidirectional), impose negligible CPU load on modern devices, and operate with 150-200ms end-to-end latency. Adding HIPAA compliance requirements introduces end-to-end frame encryption (+15% CPU, +30ms latency), comprehensive audit logging (200 log entries over the session), encrypted session recording (1.2GB storage, +10% CPU), and multi-factor authentication overhead at session start.
The result: Total latency increases to 180-250ms (still acceptable for conversation), CPU usage on the provider’s device increases by 25-30%, but the patient experience remains largely unchanged. The primary impact is on the provider’s device and backend infrastructure.
Scenario 2: Multi-Party Specialist Consultation
- Primary care physician, specialist, patient, and medical interpreter
- 45-minute consultation
- Multiple screen shares (X-rays, lab reports, EHR screens)
- High-resolution video for detailed visual examination
This scenario stresses the system significantly more. The media server must route four video streams, manage multiple screen shares, handle end-to-end encryption for all participants, and log participant actions in real-time. Without optimization, the combined overhead can push latency above 500ms and cause noticeable quality degradation.
Successful implementation requires selective video quality reduction (patient sees provider in HD, provider sees patient in HD, other participants receive SD), dedicated media servers for multi-party sessions, and optimized logging that batches non-critical events while immediately persisting security-relevant actions.
Scenario 3: Behavioral Health Session from Low-Bandwidth Environment
- Therapist in office, patient at home with limited internet (5 Mbps down, 1 Mbps up)
- 50-minute session
- Recording required for insurance documentation
This scenario highlights how compliance overhead impacts constrained environments. The patient’s limited upload bandwidth becomes the bottleneck, and any additional overhead from encryption or quality-of-service monitoring can push the connection beyond its capacity. Success requires aggressive bitrate adaptation (reducing quality to match available bandwidth), audio-prioritized fallback (maintain audio quality, reduce video to slideshow if necessary), and client-side recording on the therapist’s system to avoid requiring patient upload of recording data.
Partnering for Compliance and Performance
Building a telemedicine platform that satisfies HIPAA requirements while delivering excellent video performance requires specialized expertise. The technical challenges are significant: implementing efficient end-to-end encryption, designing scalable audit logging infrastructure, optimizing recording strategies for various clinical scenarios, and managing encryption key lifecycles securely all demand deep knowledge of both real-time communications and healthcare compliance.
This is where working with an experienced technology partner becomes essential. Trembit brings extensive expertise in building WebRTC-based telemedicine platforms that balance compliance with performance. Our team understands the nuances of HIPAA requirements and has successfully implemented encryption, logging, and recording architectures that meet regulatory standards without sacrificing the user experience.
We work closely with healthcare organizations to design solutions tailored to their specific clinical workflows and compliance requirements. From architecture design through deployment and ongoing optimization, Trembit provides the technical depth and healthcare industry knowledge needed to navigate the compliance-performance tradeoff successfully.
Finding the Balance
The conflict between HIPAA compliance and WebRTC performance is real, but it’s not insurmountable. Success requires careful architectural decisions that prioritize what matters most for patient care, strategic implementation of compliance measures that minimize performance impact, continuous monitoring and optimization of both security and performance metrics, and realistic expectations about the tradeoffs inherent in secure, compliant telemedicine.
The organizations that succeed are those that treat compliance not as a checkbox exercise but as an integral part of system design. By building security and audit capabilities into the architecture from the beginning rather than bolting them on afterward, it’s possible to create telemedicine platforms that protect patient privacy while delivering the high-quality, low-latency video experience that effective healthcare requires.
The technical challenges are significant, but the stakes are higher. Telemedicine has the potential to expand access to healthcare, improve outcomes, and reduce costs — but only if platforms are both compliant and usable. Finding the balance between these competing demands is the key to realizing that potential.
About This Article: This analysis explores the technical challenges of building HIPAA-compliant telemedicine platforms using WebRTC, focusing on the performance implications of required security measures. For more insights on healthcare technology solutions, visit trembit.com.
Building a telemedicine platform? Trembit’s team has deep experience implementing WebRTC solutions that meet HIPAA requirements while maintaining excellent performance. Contact us to discuss your compliance and performance challenges and learn how we can help deliver a telemedicine platform that works reliably for both providers and patients.