Group therapy sessions represent one of the most challenging use cases for WebRTC video conferencing platforms. Unlike corporate meetings, where participants can tolerate occasional quality degradation, therapy sessions demand consistent audio clarity and reliable visual connection — the foundation of therapeutic rapport. However, many healthcare organizations discover too late that their video platform performs beautifully with four participants but becomes unusable at six. This isn’t a bug — it’s a fundamental architectural inflection point where multiple technical constraints converge.
Understanding why six participants create such a dramatic scaling cliff is essential for anyone building or procuring telemedicine platforms for behavioral health. The answer involves client-side fan-out mathematics, audio mixing complexity, asymmetric bandwidth limitations, and mobile device resource constraints that all reach critical thresholds simultaneously.
The Deceptive Simplicity of Small Groups
Four-person group therapy sessions work remarkably well with standard WebRTC implementations. A therapist and three clients can connect reliably, maintain eye contact through video, and conduct effective sessions with minimal technical intervention. The video quality is good, audio is clear, and even participants joining from home networks experience acceptable performance.
Then the organization adds one more participant to sessions — perhaps, integrating a family member or accommodating a slightly larger therapy group — and everything falls apart. Video becomes choppy, audio cuts in and out, mobile participants drop from sessions, and the therapist spends more time troubleshooting technology than facilitating therapy. What changed?
The transition from five to six participants crosses multiple technical thresholds simultaneously, creating a perfect storm of resource exhaustion. To understand this phenomenon, we need to examine how WebRTC architectures handle small group calls and where they break down.
SFU Fan-Out: The Mathematical Reality
Most modern video platforms use the Selective Forwarding Unit architecture for group calls. In an SFU topology, each participant uploads their video and audio stream once to a central media server, which then forwards these streams to all other participants. This approach is far more efficient than peer-to-peer mesh networks, where each participant would need to upload their stream separately to every other participant.
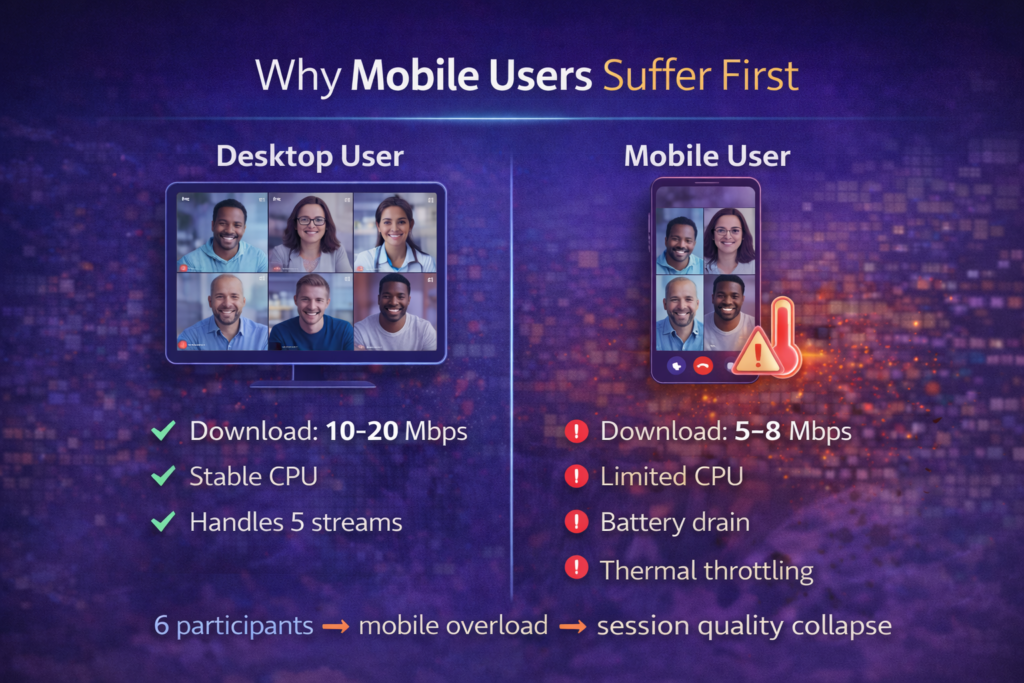
However, SFU architecture introduces asymmetric bandwidth requirements — participants need significantly more download capacity than upload capacity. Consider the mathematics of a six-person group therapy session. Each participant uploads one video stream (their own) but downloads five video streams (everyone else’s). If each video stream consumes 1.5 Mbps, the upload requirement is manageable at 1.5 Mbps, but the download requirement jumps to 7.5 Mbps.
This asymmetry creates problems because typical home and mobile internet connections are asymmetric in the opposite direction. A home connection might offer 10 Mbps upload but only 5 Mbps download, making it bandwidth-constrained on the receiving side despite having plenty of upload capacity. Research shows that in SFU-based calls, the downlink rate is approximately 2-3 times higher than the uplink rate, and this ratio increases with participant count.
The transition from five to six participants pushes many connections beyond their download capacity threshold. Five incoming streams totaling 6.25 Mbps might work, but six streams requiring 7.5 Mbps exceed available bandwidth. WebRTC’s congestion control responds by reducing video quality, but this quality reduction affects all streams, not just the marginal sixth stream, degrading the entire session experience.
Moreover, client devices must decode and render all incoming video streams simultaneously. Modern devices can typically handle 4-6 simultaneous video decodes efficiently before becoming CPU-bound. At six participants, devices are operating at the edge of their decoding capability, leaving no headroom for quality spikes or additional processing demands.
| Participant Count | Uplink Requirement | Downlink Requirement | Client Video Decodes | Typical Home Internet Adequacy |
| 2 (1-on-1) | 1.5 Mbps | 1.5 Mbps | 1 stream | Excellent |
| 4 participants | 1.5 Mbps | 4.5 Mbps | 3 streams | Good |
| 6 participants | 1.5 Mbps | 7.5 Mbps | 5 streams | Marginal |
| 8 participants | 1.5 Mbps | 10.5 Mbps | 7 streams | Poor |
| 10 participants | 1.5 Mbps | 13.5 Mbps | 9 streams | Very Poor |
These numbers assume 1.5 Mbps per stream at moderate quality (720p at 30fps). Higher quality video or additional features like screen sharing multiply these requirements accordingly.
Audio Mixing: The CPU Silent Killer
While everyone focuses on video bandwidth, audio processing often becomes the hidden bottleneck in six-participant calls. Unlike video, where displaying one stream at a time is acceptable, audio requires mixing all active speakers’ voices into a coherent soundscape. This mixing happens on the client side in SFU architectures, consuming CPU cycles that many people don’t account for.
In a four-person session, mixing three incoming audio streams is computationally trivial — even modest devices handle this easily. However, audio mixing complexity doesn’t scale linearly. Mixing five audio streams in a six-person session requires significantly more processing because the algorithm must handle multiple simultaneously speaking participants, apply echo cancellation for each stream, perform noise suppression, and synchronize audio across streams with varying latency.
The challenge intensifies because therapy sessions involve frequent overlapping speech. Unlike corporate meetings, where cultural norms discourage interruption, therapy groups often feature multiple participants speaking simultaneously — supporting comments, emotional reactions, or therapeutic interventions that overlap naturally. This means the audio mixer cannot take shortcuts like only processing the loudest three speakers, a common optimization that works well for corporate calls but fails for therapy sessions where all voices matter clinically.
WebRTC’s audio processing pipeline includes several computationally intensive stages. For each incoming audio stream, the system performs packet jitter buffering to smooth network irregularities, decoding using the Opus audio codec, echo cancellation to prevent feedback loops, noise suppression to remove background sounds, and mixing with other active audio streams. Each stage consumes CPU resources, and with five incoming streams, this processing can consume 15-30% of available CPU capacity on typical devices.
This CPU overhead accumulates with the video decoding load. When a device is simultaneously decoding five video streams (consuming 40-60% CPU) and mixing five audio streams (consuming 20-30% CPU), total CPU utilization approaches 80-90%. At this utilization level, devices struggle to maintain consistent performance, leading to audio dropouts, video frame drops, and increased latency.

The Audio Mixing Optimization Problem
Several strategies can reduce audio mixing overhead, but each involves tradeoffs:
- Server-side audio mixing: Move mixing to the server, which combines all audio into a single stream sent to each participant. This approach eliminates client-side mixing overhead but introduces latency (20-50ms additional delay) and eliminates spatial audio cues that help participants distinguish speakers.
- Active speaker limitation: Only mix the N loudest speakers (typically three), ignoring quieter participants. This drastically reduces CPU load but is clinically unacceptable for therapy where every participant’s voice matters, including soft-spoken clients or participants having emotional reactions.
- Selective audio forwarding: Forward only audio streams that exceed a volume threshold, using discontinuous transmission for silence periods. This reduces network bandwidth and mixing overhead but can miss therapeutically significant quiet speech or emotional moments.
- Optimized mixing algorithms: Use SIMD instructions (SSE, AVX) to accelerate mixing operations. Modern implementations show 30-50% reduction in audio processing overhead, but require careful optimization and don’t work on all devices.
The optimal approach for behavioral health applications typically involves selective optimization—implementing efficient mixing algorithms while preserving all clinically relevant audio, even at the cost of some additional CPU usage.
Uplink Asymmetry: The Mobile Bottleneck
The bandwidth asymmetry problem becomes particularly severe for mobile participants. While home broadband connections typically offer adequate download speeds, mobile connections often have significantly constrained upload bandwidth, especially in areas with poor cellular coverage — precisely where many therapy clients live.
A therapy client joining from their smartphone on a marginal LTE connection might have 10 Mbps download available but only 2-3 Mbps upload. In a six-person session, they need to upload their own 1.5 Mbps video stream while downloading five incoming streams totaling 7.5 Mbps. The download side works, but their upload bandwidth is adequate with little room for quality spikes or network congestion.
The situation worsens when we consider that WebRTC’s congestion control algorithm prioritizes maintaining connection stability over video quality. When the system detects bandwidth constraints, it begins aggressively reducing video resolution and frame rate. For a mobile participant with constrained upload, this means their video feed degrades significantly, impacting their ability to establish therapeutic rapport through visual connection.
Moreover, mobile devices introduce additional constraints beyond bandwidth. Smartphones must balance video encoding/decoding with battery consumption, thermal management, and other background processes. A six-person video call can drain a smartphone battery in 90 minutes and cause noticeable device heating. For therapy sessions that may last 60-90 minutes, this creates practical usability problems.
Research on mobile WebRTC performance shows that mobile platforms limit video resolution to 640×480 at 30fps even when cameras support higher resolutions, and iOS and Android behave similarly across performance characteristics. This limitation exists to balance quality with device capabilities, but it means mobile participants inherently operate at lower quality than desktop users, creating an unequal visual experience that can be therapeutically problematic.
Mobile-Specific Optimization Strategies
Several approaches can improve mobile participant experience:
- Adaptive resolution per participant: Desktop users receive higher-quality streams while mobile users receive optimized lower-resolution streams. This requires server-side transcoding or simulcast with intelligent stream selection.
- Audio-prioritized fallback: When mobile bandwidth becomes constrained, automatically degrade video to slideshow rates (1-5 fps) while maintaining audio quality. Therapy can continue effectively with static video and clear audio.
- Battery optimization modes: Offer mobile users the option to disable their outgoing video while maintaining incoming video viewing. This reduces encoding overhead and extends battery life significantly.
- Progressive quality reduction: Start mobile participants at lower quality settings proactively rather than waiting for congestion to trigger quality reduction. This provides a more consistent experience.
Mobile Degradation: The Hidden Tax
Beyond bandwidth constraints, mobile devices face computational limitations that desktop systems don’t encounter. A typical therapy group might include one therapist on a desktop workstation, two clients on laptops, and three clients on smartphones. The desktop and laptop users experience acceptable performance, but mobile users struggle with choppy video, audio delays, and frequent disconnections.
This disparity creates therapeutic challenges. When some participants experience poor quality while others see clear video, it creates an unequal therapeutic environment. A mobile participant experiencing frequent disconnections may disengage from the session, reducing therapeutic effectiveness. The therapist must choose between slowing down to accommodate technical difficulties or continuing the session while some participants struggle.
The technical causes of mobile degradation are multifaceted:
Thermal throttling: Sustained video encoding/decoding generates heat. After 15-20 minutes of continuous operation, mobile processors begin thermal throttling, reducing clock speeds to manage temperature. This manifests as progressively degrading video quality and increased frame drops.
Background process competition: Mobile operating systems aggressively manage background processes to preserve battery life. A therapy app might lose processing priority if notifications arrive, other apps request resources, or the OS decides to prioritize system functions.
Network handoffs: Mobile participants moving between WiFi and cellular, or between cellular towers, experience brief connection interruptions. WebRTC handles these relatively well, but in a six-person session operating near capacity, these handoffs often trigger cascading quality reduction across all streams.
Memory pressure: Decoding five simultaneous video streams requires significant memory. On devices with limited RAM (common in budget smartphones), the OS may kill background processes or even force the browser to reload, dropping the participant from the session entirely.
Organizations serving populations with limited resources—a common scenario in behavioral health — must design for lowest-common-denominator devices. If significant portions of clients use older or budget smartphones, the six-participant threshold may actually be lower, perhaps at four or five participants, depending on device capabilities.
Designing for Small-Group Reality
Understanding these constraints allows us to design video platforms that work reliably for group therapy. The goal isn’t to support unlimited participants in every session, group therapy rarely exceeds 8-10 participants anyway, but rather to provide consistent, clinically adequate quality within realistic constraints.
Architecture Patterns for Small Groups
Several architectural approaches address the six-participant scaling cliff:
Simulcast with Intelligent Selection: Configure clients to upload multiple quality versions of their video (high, medium, low resolution). The SFU selects appropriate quality for each recipient based on their available bandwidth and device capabilities. Desktop users receive high quality, and mobile users receive optimized streams. This approach adds upload overhead (sending multiple streams) but provides much better per-recipient optimization.
Hybrid SFU-MCU with Active Speaker Emphasis: Maintain SFU topology for the therapist and most engaged participants (active speakers) while using MCU-style composition for passive participants. This provides low-latency, high-quality video for therapeutic dyads while efficiently serving observers at lower computational cost.
Dynamic Participant Limits: Implement intelligent session management that analyzes participant device capabilities and connection quality before allowing additional participants to join. If existing participants are experiencing quality issues, prevent additional joins until conditions improve.
Bandwidth Pre-flight Checks: Before sessions begin, conduct quick bandwidth tests for each participant and adjust video quality settings proactively. A client with 3 Mbps download should start at lower resolution rather than beginning at high quality and degrading mid-session.
Audio Architecture for Clarity
Audio quality is non-negotiable in therapy. Several approaches ensure clear audio even in challenging scenarios:
- Separate audio and video optimization: Treat audio and video bandwidth as independent allocations. Reserve 256-512 Kbps per participant for audio (significantly higher than typical WebRTC settings) and adjust video quality to fit remaining bandwidth. This ensures speech clarity even when the video degrades.
- Server-side noise suppression: Implement noise suppression on the server before forwarding streams, reducing CPU load on receiving clients. Modern AI-based noise suppression can dramatically improve audio quality in challenging acoustic environments.
- Dynamic audio routing: For participants experiencing CPU constraints, selectively reduce the number of audio streams they receive by applying aggressive voice activity detection. Only forward audio from participants who are actively speaking.
- Opus codec optimization: Configure the Opus audio codec for speech-optimized settings rather than music settings. Speech optimization reduces bitrate requirements by 30-40% while maintaining clarity for voice communication.
Mobile-First Design Principles
Given that many therapy clients participate via mobile devices, design with mobile constraints as the primary consideration:
- Default mobile participants to 480p video at 15-24 fps instead of 720p at 30 fps
- Implement aggressive battery optimization with clear indicators when video quality is reduced to preserve battery
- Provide offline fallback for session notes and scheduling, so brief disconnections don’t disrupt the entire session
- Design UI with large touch targets and minimal on-screen controls to reduce cognitive load during therapeutic moments
- Test extensively on budget Android devices and older iPhones, not just flagship models
Partnering for Clinical-Grade Video
Building a video platform that handles the complexities of group therapy requires specialized expertise in both real-time communications and healthcare workflows. The technical challenges are significant: optimizing SFU fan-out for constrained connections, implementing efficient audio mixing that preserves clinical relevance, managing mobile device limitations without degrading therapeutic experience, and balancing quality with reliability across diverse participant devices and network conditions.
This is where partnering with an experienced technology provider becomes essential. Trembit brings deep expertise in building WebRTC platforms that handle the unique demands of healthcare applications. Our team understands the clinical requirements of behavioral health and has successfully implemented video architectures that maintain quality and reliability at critical participant thresholds.
We work closely with behavioral health organizations to design solutions that prioritize therapeutic effectiveness while managing technical constraints. From architecture design through deployment and ongoing optimization, Trembit provides the technical depth and healthcare industry knowledge needed to build group therapy platforms that work reliably for therapists and clients alike.
The Path Forward
The six-participant scaling cliff is real, but it’s not insurmountable. Success requires understanding that this threshold represents the convergence of multiple technical constraints, accepting that small-group calls have fundamentally different requirements than large meetings, and designing architecture that prioritizes clinical effectiveness over feature maximization.
Organizations building or procuring group therapy platforms should explicitly test with six participants using representative devices and network conditions. Don’t assume that performance at four participants predicts performance at eight. The inflection point matters.
More importantly, recognize that “supporting up to 12 participants” means something very different from “providing clinically adequate quality for 12 participants.” Marketing claims about maximum participant counts rarely account for real-world device diversity, network variability, or the audio clarity requirements that make therapy effective.
The behavioral health industry deserves video platforms designed for its specific needs — platforms that prioritize every participant’s voice, maintain quality on budget mobile devices, and scale gracefully rather than falling off a cliff at arbitrary participant counts. Building these platforms requires acknowledging the technical constraints, designing around them intelligently, and partnering with experts who understand both the technology and the clinical context.