AI in healthcare in 2026 runs in production at scale in four places: ambient clinical documentation (AI scribes), imaging-triage support for radiologists, administrative and back-office automation (prior authorization, claims, scheduling), and retrieval-grounded clinical-knowledge copilots that answer clinician questions from a defined source library. What is not running in production anywhere at scale is AI making autonomous diagnoses or treatment decisions without a clinician in the loop. Trembit builds and integrates these systems — and the compliant platform they run on. We build the compliant platform AI runs on, not the model: we do not train diagnostic or foundation models, and we make no clinical decisions.
Key takeaways
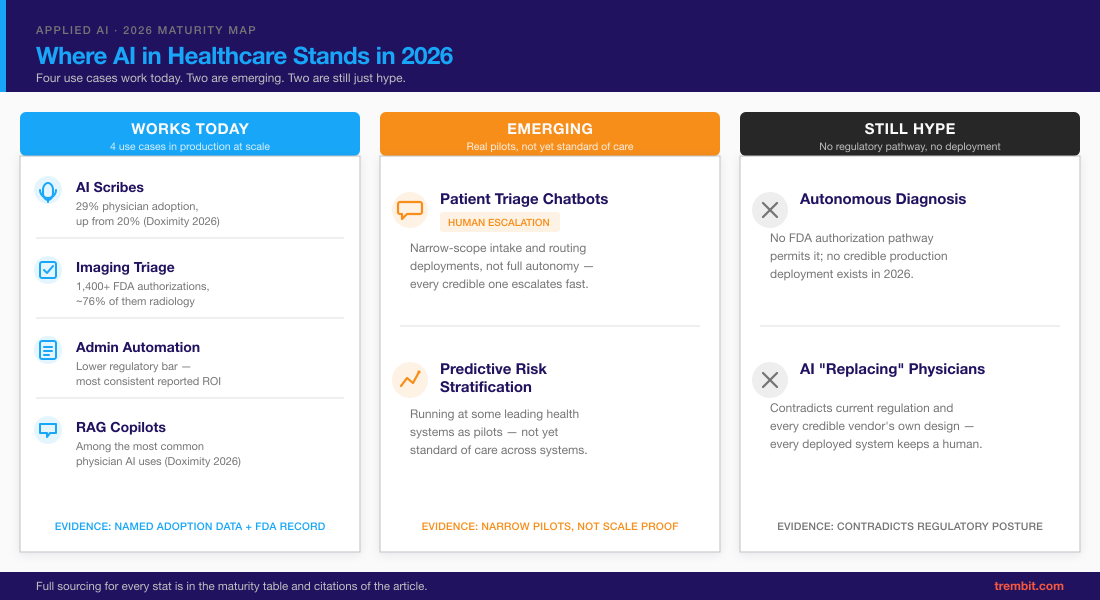
– Four AI use cases are genuinely in production at scale in 2026: ambient clinical documentation / AI scribes, medical-imaging triage support, administrative / back-office automation, and retrieval-grounded clinical-knowledge copilots.
– Autonomous diagnosis and unsupervised clinical decision-making are not in production anywhere at scale — every deployed system keeps a clinician in the loop, by design and by regulation.
– The FDA has authorized 1,400+ AI/ML-enabled medical devices cumulatively (1,451 through the end of 2025), with radiology accounting for roughly three-quarters of them — but each authorization covers a narrow, defined function, not general clinical judgment.
– Physician AI adoption reached 63% in the 2026 Doximity survey, up from 47% a year earlier; ambient/voice documentation is the second most common use case at 29% (up from 20%).
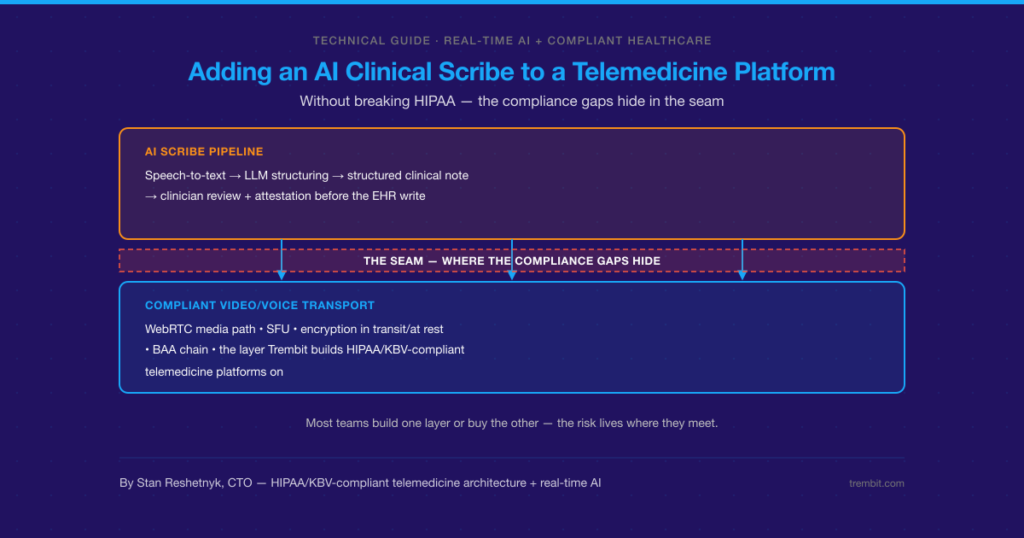
– The real bottleneck to scaling healthcare AI isn’t model quality — it’s compliant integration: EHR write-back, HIPAA/BAA coverage, audit trails, and a defensible human-in-the-loop design.
– Trembit builds and integrates AI-powered healthcare systems and the compliant platform underneath them — not diagnostic or foundation models, and we hold no clinical or device clearance.
What Does “AI in Healthcare” Actually Mean in 2026?
“AI in healthcare” covers three distinct layers, and most of the confusion in the market comes from collapsing them into one. The first is clinical and patient-facing AI — documentation, imaging triage, symptom intake, and clinician copilots. The second is operational AI — the back-office automation that never touches a diagnosis: prior authorization, claims coding, scheduling, intake processing. The third, and the one buyers underestimate most, is the infrastructure layer — the compliant platform that both of the others have to run on: EHR integration, HIPAA and Business Associate Agreement coverage, audit trails, and human review.
Throughout this piece we use one lens: works today, emerging, or still hype. “Works today” means production deployments at scale with named evidence. “Emerging” means real pilots and narrow early deployments that are not yet standard of care. “Still hype” means claims that current regulation and every credible vendor’s own posture contradict. This piece is US-primary; UK volume for the same topic is smaller but the maturity picture is the same.
Where Is AI in Healthcare Actually Working in Production Today?
Four categories clear the “works today” bar. Each entry below names the use case, its production maturity, a sourced number, and an honest caveat.
Ambient Clinical Documentation and AI Scribes — What’s Actually Confirmed?
An AI scribe listens to a clinical encounter, produces a structured draft note, and pushes it into the EHR — where the clinician reviews, edits, and signs it. The AI writes a draft; a human owns the record.
This is the fastest-moving category in the market. In Doximity’s 2026 State of AI in Medicine report, overall physician AI adoption reached 63% (up from 47% a year earlier), and voice-based/ambient documentation was the second most common use case at 29%, up from 20% the prior year. Health systems report operational gains alongside that adoption: Kaiser Permanente reported roughly 2.5 million ambient-AI-scribe encounters across 7,260 of its physicians, and Intermountain Health reported a roughly 27% reduction in documentation time using an ambient tool.
The honest caveat is a compliance one, not a quality one: audio as a data modality is not automatically covered under every vendor’s Business Associate Agreement. Whether a given scribe’s audio pipeline is HIPAA-covered is a per-vendor, per-contract question — a real integration risk, not fear-mongering. We treat that gap in depth in our clinical-AI deployment guide.
Medical Imaging Triage — Where AI Actually Helps Radiologists (and Where It Doesn’t)
Radiology is where regulatory-grade AI is most mature. The FDA’s list of AI/ML-enabled medical devices passed 1,400+ cumulative authorizations (1,451 through the end of 2025), and radiology accounts for roughly three-quarters (~76%) of every device on that list. Independent tracking put 2025 among the most active years on record for these authorizations.
Precision matters in how you read that. These are narrow, task-specific authorizations — flagging a likely abnormality for radiologist review, prioritizing a worklist, measuring a defined structure. None of them authorize autonomous diagnosis. A radiologist still reads and signs every case. An FDA authorization for a narrow triage function is not “FDA-approved AI diagnosis,” and the two should never be used interchangeably. Where imaging AI helps is throughput and prioritization; where it does not help is replacing the read.
Administrative and Back-Office Automation — the Quiet Majority of Healthcare AI ROI
The least glamorous category is where the most consistent, measurable return shows up: prior authorization, claims processing and coding assistance, scheduling, intake-form handling, and documentation summarization. The stakes are lower and the regulatory bar is lower — most of this work falls outside Software-as-a-Medical-Device regulation entirely (HIPAA still applies) — so it reaches production faster and its ROI is easier to attribute.
This is the same class of agentic, auditable back-office automation we build as AI business-tools development in other regulated industries. In fintech leasing, Trembit built an explainable ML risk-scoring pipeline for Eska with a human-review workflow and ERP integration — automated decisioning that stays explainable and auditable, with a person in the loop. The underlying pattern — explainable, auditable, human-reviewable decisioning — is the same discipline in healthcare operations; what differs is the data model and the compliance surface (payer-specific rules, X12/FHIR formats, and HIPAA-grade audit trails rather than financial ones). The principle generalizes; the specifics you engineer around do not.
Retrieval-Grounded Clinical Knowledge Copilots — Answering Clinician Questions Safely
Clinicians increasingly use AI to answer point-of-care knowledge questions — “what’s the current guidance on X” — and literature search is among the most common physician AI uses in the 2026 surveys.
The architecture is what makes this safer. Retrieval-augmented generation (RAG) grounds each answer in a defined, current, sourced knowledge base rather than the model’s parametric memory. That reduces — but does not eliminate — fabrication on factual questions, because it constrains the model to a curated source set: retrieval quality and citation fidelity become the new failure modes you engineer around. A model can still misread or mis-cite a correctly retrieved passage, and stale or conflicting source documents degrade the answer. So this is an architecture decision, not a model-choice decision: the same base model is more trustworthy when its answers are constrained to a curated corpus with citations, and less trustworthy when the retrieval layer is sloppy. Building that retrieval and grounding layer is exactly what an orchestration layer is for.
Patient Communications and Triage — Where Human-in-the-Loop Still Rules
Symptom-intake chatbots, appointment triage and routing, and post-visit follow-up messaging are in genuine production use — but at narrow scope. We classify this emerging, not “works today,” because every credible deployment keeps the AI inside intake and routing (not diagnosis) and keeps a fast, explicit escalation path to a human. Consent and liability framing govern this category: an intake bot that routes a patient is a very different regulatory object from one that advises them. The production-safe versions stay firmly on the routing side of that line.
| Use case | 2026 status | Evidence |
|---|---|---|
| Ambient clinical documentation / AI scribes | Works today | 29% physician adoption, up from 20% (Doximity 2026) |
| Medical imaging triage support | Works today (narrow, task-specific) | 1,400+ FDA AI/ML device authorizations, ~76% radiology |
| Administrative / back-office automation | Works today | Lower regulatory bar, most consistent reported ROI |
| Retrieval-grounded clinical knowledge copilots | Works today | Among the most common physician AI uses (Doximity 2026) |
| Patient triage / intake chatbots | Emerging | Narrow-scope, human-escalation deployments, not full autonomy |
| Predictive risk stratification across systems | Emerging | Health-system pilots; not yet standard of care |
| Autonomous diagnosis without clinician review | Still hype | No FDA authorization framework permits it; no credible production deployment |
| AI “replacing” physicians / fully autonomous clinical agents | Still hype | Contradicts current regulation and every credible vendor’s own claims |
Notice what every “works today” row has in common: none of them is a smarter model. Each one clears the bar because someone solved the boring part — EHR write-back, HIPAA coverage, audit trails, human review. That is the whole game, and it is where we work.
We build the compliant platform AI runs on — not the model.
We proved that at scale on the Martti medical-interpretation platform for Equiti Health — a HIPAA/SOC 2 system integrated into Epic, Oracle Cerner, and eClinicalWorks across 4,000+ healthcare facilities at 99.99% uptime. It is not an AI product, but it is exactly the kind of compliant, EHR-integrated foundation a production AI feature has to sit on.
Evaluating how to bring AI into a compliance-gated healthcare product? Trembit builds the integration and compliance layer this requires. Talk to our team about building AI into your healthcare product.
Where Is AI in Healthcare Still Emerging, Not Yet Production-Ready?
Several categories are real but not yet proven at production scale the way the four above are. Multi-agent care-coordination systems — where AI agents hand tasks to one another across a care pathway — exist in pilots but not as standard operations. Personalized treatment-plan generation is being tested as clinician-facing decision support, always with sign-off, never as an autonomous prescriber. Predictive risk stratification deployed across whole systems — flagging deterioration or readmission risk across a full patient population — runs at some leading health systems but is not yet standard of care, and its real-world performance varies by setting and data quality.
The honest framing: pilots and early deployments exist, and some are promising, but “a model performs well in a pilot” and “a system is safely running in live clinical workflows” are two different achievements. We describe categories here rather than naming specific vendor pilots, because unverified pilot claims are exactly the noise this piece exists to cut through.
Where Is “AI in Healthcare” Still Just Hype in 2026?
Four narratives are overclaimed, and the regulatory reality already covered above is enough to debunk them without opinion. AI autonomously diagnosing patients has no authorization pathway — the FDA authorizes narrow, defined functions, not general clinical judgment, so a system that diagnoses and decides on its own has no route to legal production use in the US. AI “replacing” physicians contradicts both regulation and the actual design of every deployed system, all of which keep a clinician in the loop. A single foundation model making end-to-end treatment decisions describes no shipping product. Fully autonomous agents acting on a patient record without human sign-off is the same claim in agentic clothing — and the same regulatory wall stops it.
None of this means the underlying technology is fake. It means the timeline and autonomy in the marketing are ahead of what is legal, safe, or deployed. The useful question for a buyer isn’t “will AI replace the clinician” — it’s “which narrow, reviewable function can I put into production this year.”
Why Doesn’t More Healthcare AI Reach Production?
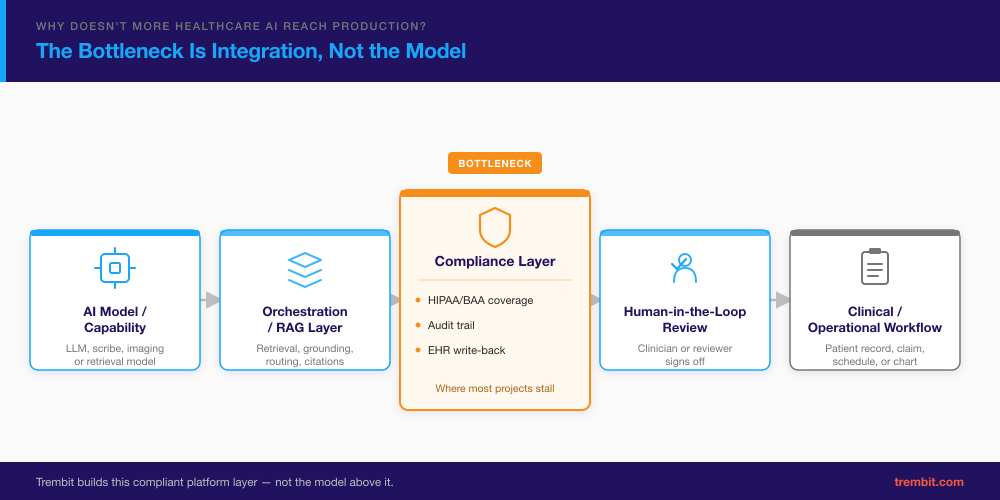
The bottleneck is almost never model quality. It’s integration. A pilot that proves a model works is a small, contained problem; getting that model safely into a live clinical or operational workflow is a much larger one — and it’s where most healthcare AI projects stall.
Four things do the stalling. EHR write-back is genuinely hard: every EHR (and every module within Epic) exposes a different integration surface, and writing structured data back into a patient record under the right permissions is not an API call. HIPAA and BAA coverage has to be established per data modality — the audio-BAA gap for scribes is one example of a coverage question that only surfaces when you try to ship. Audit trails and explainability are not optional: any AI decision that touches a patient record has to be reconstructable after the fact. And human-in-the-loop design has to be built in, not bolted on, or the whole system fails its own compliance review.
We learned the general version of this lesson building the platform behind Equiti Health’s Martti medical-interpretation platform — a WebRTC video-interpretation system serving 4,000+ healthcare facilities, integrated into Epic, Oracle Cerner, and eClinicalWorks, under HIPAA and SOC 2, at 99.99% uptime. The hard-won principle from that build: EHR integration is an architecture decision, not a feature addition. Teams that build a core system first and “add EHR later” end up rebuilding significant portions.
That principle is not AI-specific — it’s why healthcare AI is hard to ship, and the same discipline carries over to an AI system, even though the specifics differ. AI-output write-back adds requirements a routing platform never had to solve: data lineage, model-version audit trails, and defined handling of low-confidence outputs. The architecture-first lesson generalizes; the integration surface is heavier. (To be precise about what Martti is: its interpreter-matching is rules- and logic-based routing on language, availability, and specialty — not clinical AI and not an AI-diagnostic system. We cite it for its EHR-integration and compliance engineering, nothing more.)
What Regulatory and Safety Frameworks Govern AI in Healthcare?
You don’t need to master this list yourself before you build — you need a partner who already has, and you need to know which framework your use case triggers before you write a line of code. Here’s the map. In the US, the FDA regulates AI/ML-enabled Software as a Medical Device (SaMD), and its Predetermined Change Control Plans (PCCPs) define how an adaptive or updating model can change post-authorization without a new submission — which is also why a deployed clinical-adjacent model is never “done” at go-live: real-world accuracy can drift as the patient population or documentation style shifts, and the PCCP is the mechanism for governing that change. HIPAA and its Business Associate Agreements govern protected health information across any system, device or not. In the UK, NHS clinical-safety standards DCB0129 and DCB0160 apply to health-IT manufacturers and deploying organizations. Globally, the WHO’s guidance on the ethics and governance of AI for health frames the safety and equity expectations. In US health IT specifically, ONC/ASTP’s HTI-1 transparency rule sets disclosure requirements for predictive AI in certified systems, and the Coalition for Health AI (CHAI) assurance framework is emerging as an industry-standard reference.
Trembit covers the practical compliance checklist — DCB0129/0160, HIPAA/BAA specifics, and audit-trail requirements — in our clinical-AI deployment guide.
How Should a Healthcare Company Approach AI Adoption in 2026?
Four principles keep an AI project on the path to production rather than the pilot graveyard.
Start where the regulatory bar is lowest and the ROI is clearest. For most organizations that is administrative automation or documentation, not diagnosis. Prove value and build institutional trust on the low-risk use case first.
Design for EHR and HIPAA integration from day one. As the Martti lesson shows, integration is architecture. Deciding how the system writes to the record, and how it stays HIPAA-covered per modality, before you build the core saves you from rebuilding it later.
Keep a clinician or reviewer in the loop for anything patient-facing. This is both a safety requirement and, in most categories, a regulatory one. The AI drafts, flags, or routes; a human decides.
Build for auditability. Every AI decision that touches a patient record should be explainable after the fact — what data went in, what came out, who reviewed it. If you cannot reconstruct a decision, you cannot defend it in a compliance review, and you should not ship it.
How Does Trembit Approach AI in Healthcare?
Our position is simple, and worth stating plainly: we build the compliant platform AI runs on — not the model. Trembit builds and integrates the AI-powered systems that healthcare and healthcare-adjacent companies put into production — LLM applications, agents, orchestration and RAG layers, and ML/data pipelines — and the compliant platform underneath them. In plain terms, we get your AI feature into production without blowing up your compliance review. We do not train proprietary foundation or diagnostic models, we do not make clinical decisions, and we hold no FDA clearance or CE mark. Our moat is engineering and integration: real-time systems, systems integration, and HIPAA/GDPR/KBV-grade compliance.
Trembit has been building this class of compliant, real-time infrastructure since 2018 (the founding team has worked together on video and voice since 2009), with about 30 people including 20-plus engineers and 50+ video and voice projects behind us — long enough to have shipped healthcare-grade systems, not a single lucky platform.
Here we should be straight about what the proof below does and doesn’t show: our cited healthcare work is compliant-platform and integration engineering, plus a cross-industry AI pattern — we have not yet shipped a named AI-in-healthcare clinical feature (a scribe, an imaging-triage integration, a RAG copilot) inside a live healthcare product. That is the honest boundary of what these references prove, and it’s consistent with everything else this piece argues: the hard part, and what we’ve done at scale, is the compliant platform underneath.
The evidence is in the compliant platforms we’ve shipped. The Martti platform for Equiti Health is our track record for exactly the “compliant platform AI has to run on” problem: 4,000+ healthcare facilities (including NYU Langone, Stanford Health, Henry Ford Health, Northwestern Memorial, and Prisma Health, named publicly on equitihealth.com), native Epic/Oracle Cerner/eClinicalWorks integration, HIPAA and SOC 2, 99.99% uptime, and rules-based language routing engineered from the WebRTC protocol level up (routing logic, not AI). In Germany, we built WebPRAX, a KBV-certified video platform for psychotherapy with Germany-only data residency and DSGVO compliance — a rare regulated-healthcare credential; we also break down what that certification requires in our guide to meeting KBV certification requirements for video consultations. And in fintech, our explainable ML risk-scoring pipeline for Eska shows the auditable, human-in-the-loop decisioning pattern — the same discipline healthcare operations need, though the data model and compliance surface differ.
If you’re evaluating how to bring AI into a clinical or healthcare-adjacent product safely, Trembit’s team can review your architecture and compliance requirements — and give you a directional read on which low-risk use case (usually documentation or admin automation) can reach production first. Start with a scoping conversation.
FAQ
What is AI actually used for in healthcare today?
Four things are in production at scale in 2026. AI scribes generate draft clinical notes from an ambient recording of the visit, which the clinician reviews and signs. Imaging AI triages and prioritizes radiology cases for a radiologist to read. Administrative AI automates prior authorization, claims coding, and scheduling. And retrieval-grounded copilots answer clinician knowledge questions from a defined source library. All four keep a human in control of the final decision. Autonomous diagnosis is not among them.
Is AI in healthcare regulated by the FDA?
Yes — for AI/ML-enabled medical devices, regulated as Software as a Medical Device. The FDA has authorized 1,400+ such devices cumulatively (1,451 through the end of 2025). But that does not mean all healthcare AI is FDA-regulated: administrative and back-office AI, and most documentation tools, typically fall outside SaMD regulation. HIPAA and other requirements still apply to those systems even when the FDA doesn’t.
Can AI diagnose patients on its own in 2026?
No. Every credible production deployment keeps a clinician in the loop. FDA authorizations cover narrow, defined functions — for example, flagging a finding for radiologist review — not autonomous diagnostic authority. There is no US regulatory pathway that permits an AI system to diagnose and decide on its own without clinician review, and no credible vendor claims one.
What’s the difference between clinical AI and AI-powered healthcare operations?
Clinical AI is patient-facing or diagnosis-adjacent — imaging triage, clinical copilots, decision support — and carries a higher regulatory bar, often SaMD. Operational AI handles the back office — scheduling, claims, prior authorization, intake — at a lower regulatory bar, which is why it reaches production faster and shows more consistent ROI. The deeper compliance framework for the clinical side (DCB0129/0160, HIPAA/BAA specifics, audit trails) is covered in our clinical-AI frameworks guide.
Why do so many healthcare AI pilots never reach production?
Because the blocker is integration, not model quality. Getting a model into a live workflow means EHR write-back, HIPAA/BAA coverage established per data modality, audit trails, and a defensible human-in-the-loop design. A pilot proves the model works in a controlled setting; production requires the model to work safely inside a clinical or operational system it wasn’t built to live in. That gap — architecture, not accuracy — is where most projects stall.
Is ambient AI documentation (AI scribes) HIPAA compliant?
It depends on the vendor and the data modality. Not every scribe product’s audio pipeline is covered under every provider’s Business Associate Agreement as of 2026 — audio as a modality can be treated differently from the resulting text note. This is a real, per-vendor question to verify contract by contract, not a blanket yes. We treat the audio-BAA gap in depth in our clinical-AI deployment guide.
AI in healthcare in 2026 is real and working — in four specific, provable places — and the honest reason more of it isn’t in production yet is integration and compliance, not model capability. If you’re deciding how to bring AI into a healthcare or healthcare-adjacent product without overstepping what’s safe or legal, talk to our team about integrating AI safely into your healthcare product.