Artificial intelligence that can read a patient’s emotional state during a telehealth consultation sounds either like a breakthrough or a surveillance concern, depending on who you ask. Proponents describe a near future where AI assistants flag signs of depression before a clinician notices them, alert providers to patient distress in real time, and generate post-consultation sentiment reports that improve care quality. Critics point to shaky science, significant bias risks, and serious ethical questions about applying affective computing in a clinical setting without patient awareness or consent.
Both sides have valid points. And somewhere between the vendor pitch decks and the academic skepticism is the reality that healthcare technology leaders actually need to navigate.
This article looks at what emotion detection technology in telehealth can and cannot do today, where the evidence is credible, where the risks are real, and what a responsible approach to implementing it looks like — if it belongs in your product at all.
What Emotion Detection Technology Actually Does
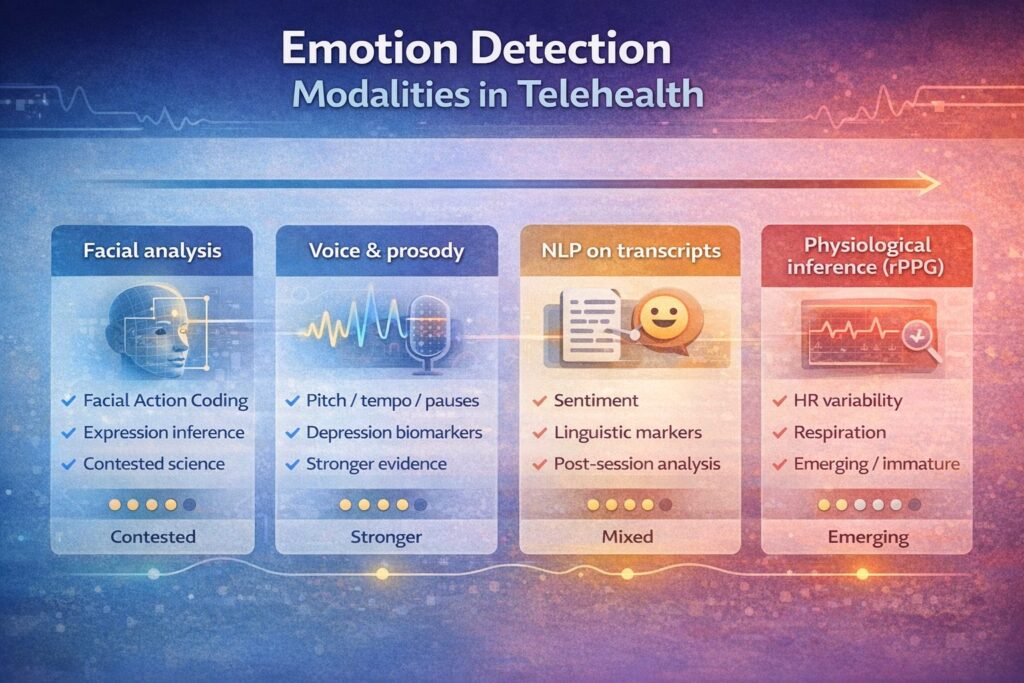
The term “emotion detection” covers a range of technologies that analyze different signal types to infer psychological or emotional states. In a telehealth video context, the main modalities are:
Facial Action Coding (FAC) and expression analysis. Computer vision models analyze facial muscle movements — the position of the brow, the corners of the mouth, eye aperture — and map them to inferred emotional states. This approach descends from Paul Ekman’s Facial Action Coding System, developed in the 1970s, which proposed a set of universal basic emotions expressed consistently through facial movements across cultures.
Voice and prosody analysis. Acoustic features of speech — pitch, tempo, energy, pauses, speech rate, and vocal tremor — are analyzed to infer emotional or psychological state. This modality is arguably more clinically grounded than facial analysis for certain conditions; changes in speech patterns are established markers in depression, mania, and Parkinson’s disease research.
Natural language processing (NLP) on transcribed speech. The content of what a patient says, not just how they say it, can be analyzed for sentiment, semantic markers of distress, or linguistic patterns associated with specific conditions. This is conceptually distinct from emotion detection but is often bundled with it in commercial offerings.
Physiological signal inference. Some systems attempt to infer heart rate variability, respiration, or skin conductance changes from video — a technique called remote photoplethysmography (rPPG). This is the most technically ambitious and least mature of the modalities.
Most commercial “emotion AI” platforms in healthcare combine several of these into a composite score or dashboard, presenting the output as a measure of patient engagement, distress, or emotional valence.
Where the Science Stands
Here, the picture becomes considerably more complicated than vendor materials suggest.
The Ekman Problem
The foundational theory behind facial emotion detection — that a defined set of basic emotions are universally expressed through consistent facial movements — has faced sustained and serious scientific criticism over the past two decades. Lisa Feldman Barrett’s work, summarized in her 2017 book How Emotions Are Made, argues that emotional expressions are highly context-dependent, culturally variable, and not reliably decodable from facial movements alone. A 2019 report from the AI Now Institute concluded that there is insufficient scientific evidence to justify deploying automated facial expression analysis for emotion recognition in high-stakes contexts.
This does not mean facial analysis has no clinical value. It means the simple mapping of facial movements to discrete emotional states — the model underlying most commercial emotion AI — is scientifically contested in ways that matter for clinical use.
Voice Analysis: Stronger Ground
The voice-based modalities have a stronger — though still imperfect — evidence base in clinical contexts. Vocal biomarker research has produced credible results for depression screening (the PRIORI project at the University of Michigan), bipolar disorder monitoring, and early Parkinson’s detection. The FDA has authorized some voice analysis tools as breakthrough devices for depression screening.
The distinction matters: voice analysis for specific, defined clinical indicators (depression, certain neurological conditions) is different from general “emotion detection.” The former is targeted, clinically validated, and tied to defined outcomes. The latter is broad, vague, and poorly validated.
Bias: A Serious, Documented Problem
Emotion recognition systems trained predominantly on certain demographic groups perform substantially worse — and differently — on others. Studies have documented that commercial facial analysis systems misclassify the emotional expressions of darker-skinned individuals at higher rates than lighter-skinned individuals, and that gender, age, and cultural background all affect accuracy.
In a healthcare context, biased emotion detection is not just a technical problem. It is a clinical equity problem. A system that more frequently flags distress in Black patients, or underdetection in elderly patients, will systematically distort clinical attention in ways that could worsen existing disparities.
What It Can Plausibly Do Well (Right Now)
Given all of the above, where does emotion detection in telehealth have genuine, defensible utility today?
Longitudinal Mood Tracking in Mental Health
The most credible current application is not real-time emotion labeling during a consultation, but longitudinal pattern detection over time. If a depression patient uses a platform regularly and their vocal characteristics shift in ways associated with worsening mood — slower speech, more pauses, lower energy — that signal may be clinically useful as one input among many.
This framing matters: not “AI reads the patient’s emotion,” but “AI tracks changes in vocal or linguistic patterns associated with a known clinical indicator, across multiple sessions.” It is more modest, more defensible, and more useful.
Engagement and Attention Proxies
Some platforms use behavioral signals — eye contact, head movement, response latency — as proxies for patient engagement during a telehealth session. This is not emotion detection in the strong sense, but it serves a real clinical need: helping clinicians identify patients who may be disengaged, confused, or distressed in ways they are not verbalizing. Used as a soft signal to prompt a clinician’s attention, not as a diagnostic output, this has practical value.
Post-Session NLP Analysis
Natural language processing of consultation transcripts — analyzing what patients said, the language patterns they used, the topics they raised or avoided — has more defensible clinical applications than real-time facial emotion analysis. Flagging linguistic markers of suicidality, identifying when a patient uses language associated with depression relapse, or summarizing emotional themes across a session are applications where the evidence base is more solid.
The Risks That Cannot Be Ignored
| Risk | Why It Matters in Healthcare |
| Scientific validity | Most commercial emotion AI is built on contested science. Clinical decisions influenced by invalid signals cause harm. |
| Demographic bias | Systems that perform differently across race, gender, and age groups will amplify healthcare disparities. |
| Informed consent | Patients in a telehealth consultation may not know their emotional state is being analyzed. This raises serious ethical and legal questions. |
| Over-reliance | Clinicians who see an “emotion score” on a dashboard may anchor to it inappropriately, displacing clinical judgment. |
| HIPAA and data scope | Behavioral and biometric data inferred from video is arguably PHI. The regulatory status of emotion AI data under HIPAA is unsettled and requires legal review. |
| False positives | An AI that incorrectly flags a patient as distressed can trigger inappropriate clinical escalation, with real consequences for the patient. |
A Framework for Responsible Evaluation
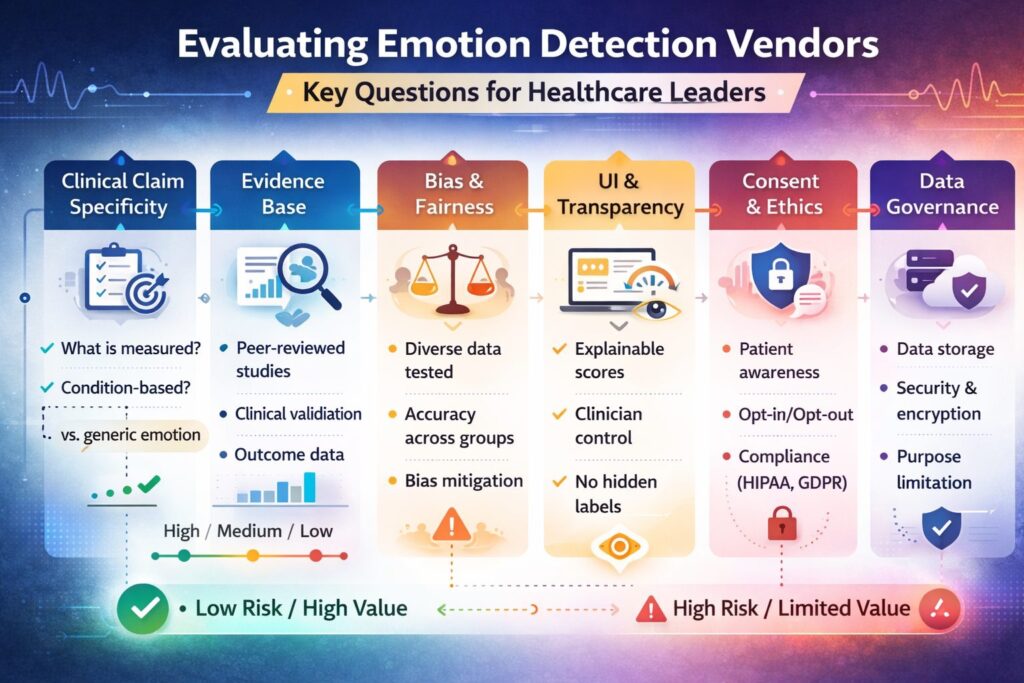
If you are evaluating emotion detection technology for a telehealth product, these questions should anchor the assessment:
What is the specific clinical claim? “Detects emotion” is not a clinical claim. “Detects vocal patterns associated with PHQ-9 score changes in patients with major depressive disorder, with a sensitivity of X and specificity of Y in a population comparable to ours” is. Demand specificity.
What is the evidence base? Published, peer-reviewed clinical validation studies, not internal benchmarks or pilot data from a proprietary dataset. Ask for the study population demographics and whether they match your patient population.
Has it been evaluated for demographic bias? Ask for disaggregated performance data by race, gender, age, and language. If the vendor cannot provide this, that is an answer.
How will it be presented to clinicians? A raw emotion score or label presented without context will be misused. Outputs should be framed as soft signals, presented with confidence intervals, and accompanied by documentation of limitations.
What does informed consent look like? Patients should know if their behavioral signals are being analyzed. Work with legal and compliance teams to determine what disclosure and consent are required in your jurisdiction.
What is the data handling model? Where is the analysis performed — on-device, on a vendor server, or in your own cloud? Who owns the inferred data? How long is it retained?
The Bottom Line: Useful in Narrow Cases, Hype in the Broad Case
Emotion detection in telehealth is not uniformly hype, but the gap between what it is marketed as and what it can responsibly deliver is wide.
The honest landscape looks like this: voice-based longitudinal mood tracking in mental health, NLP-based pattern analysis of consultation transcripts, and behavioral engagement signals used as soft clinician prompts all have credible, defensible applications. Broad, real-time facial emotion labeling applied to general telehealth consultations does not — not with the current science, not without addressing the bias problem, and not without patient consent frameworks that most platforms have not built.
The organizations that will use this technology well are those that resist the broad framing (“AI that understands your patients’ emotions”), choose the narrow, well-validated application that fits a specific clinical need, and implement it with the rigor — clinical, technical, ethical, and legal — that any clinical tool deserves.
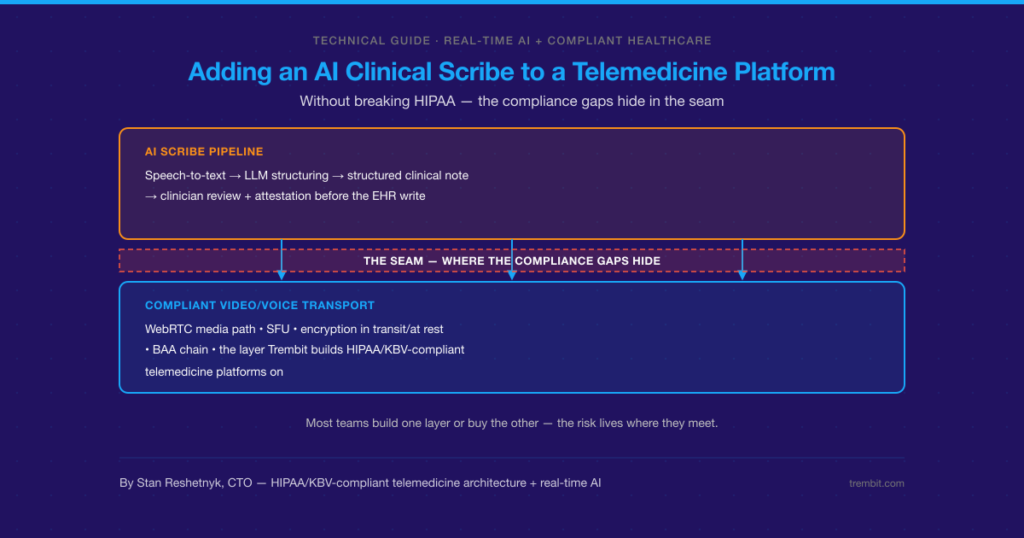
Building It Right: Where Trembit Comes In
Implementing emotion detection or behavioral signal analysis in a telehealth platform is a complex engineering and compliance challenge. The technical work — integrating audio or video analysis pipelines, processing streams in real time or near-real time, storing outputs in a HIPAA-compliant data model, surfacing signals in a clinician interface without creating inappropriate decision anchors — requires expertise across multiple disciplines simultaneously.
Trembit has built telehealth platforms and clinical data pipelines that handle exactly this kind of sensitive, high-stakes integration. We bring the engineering depth to implement AI signal pipelines correctly, the compliance architecture experience to handle behavioral and biometric data within HIPAA’s requirements, and the product judgment to help healthcare organizations distinguish between a feature that adds clinical value and one that adds liability.
If your organization is evaluating emotion detection or behavioral AI for a telehealth product — or if you want an honest technical and clinical assessment of what a vendor is proposing — Trembit is the partner to have that conversation with.
Conclusion
Emotion detection technology sits at a genuine inflection point in healthcare: past the earliest experimental stage, but well short of the broad clinical readiness that some vendors imply. The science is contested in important ways, the bias risks are documented and serious, and the ethical questions around consent and data ownership are unresolved in most deployment contexts.
None of that means it has no place in telehealth. It means the place it has is specific, narrow, and requires a level of clinical and technical rigor that hype-driven adoption skips over.
The right question is not “should we use emotion detection?” It is “for which specific clinical problem, in which patient population, with which validated tool, under which consent and governance framework?” Ask that question precisely, and the answer becomes navigable.