Building a telehealth application for a single clinic is straightforward. Building a multi-tenant telehealth architecture that serves hundreds of clinics across multiple states — each with unique workflows, compliance requirements, and branding — while maintaining security, performance, and operational efficiency, is an entirely different challenge.
Most telehealth architecture content focuses on single-provider scenarios: one database, one deployment, one set of users. But CTOs at scaling healthcare SaaS companies face fundamentally different problems. How do you ensure one clinic’s patient data never leaks to another? How do you comply with healthcare regulations across different states and countries? How do you give each clinic autonomy while maintaining centralized visibility? How do you deploy features to specific customer segments without fragmenting your codebase?
These aren’t theoretical concerns. They determine whether your platform can scale profitably, whether enterprise customers will trust you with their data, and whether your engineering team can move fast or drown in complexity. The architecture decisions you make early create constraints, or opportunities, that compound over time.
Understanding Enterprise Telehealth Requirements
Enterprise healthcare organizations evaluating telehealth platforms have requirements that go far beyond features. They’re assessing architectural maturity, operational sophistication, and long-term viability.
A hospital network acquiring your platform isn’t just buying video consultation software. They’re integrating a critical piece of infrastructure into complex existing systems — Electronic Health Records, Single Sign-On providers, HR systems, billing platforms, and clinical workflow tools. They need guarantees for data isolation, compliance certifications, uptime commitments, and disaster recovery capabilities.
Multi-clinic deployments introduce organizational complexity. Different clinics within the same enterprise may have different specialties, workflows, and regulatory requirements. A mental health clinic has different documentation needs than urgent care. A clinic in California faces different privacy regulations than one in Texas. Your architecture must accommodate this heterogeneity without creating operational chaos.
The economics change at scale. Per-clinic infrastructure costs that seem reasonable for ten customers become prohibitive at hundreds. You need architectural efficiency that allows you to serve more clinics without linear infrastructure growth. You also need operational efficiency — your support and DevOps teams can’t scale linearly with customer count.
Tenant Isolation Models: Choosing Your Foundation
Tenant isolation is the architectural foundation of multi-tenant SaaS. It determines security boundaries, compliance capabilities, performance characteristics, and operational complexity. There’s no universal right answer — the optimal model depends on your customer profile, compliance requirements, and growth trajectory.
Database-Per-Tenant Isolation
The most stringent isolation model gives each clinic its own dedicated database. Patient data for Clinic A exists in a completely separate database from Clinic B. This provides the strongest security guarantees and the clearest compliance story. If a vulnerability compromises one database, others remain unaffected. If a regulatory audit requires you to produce all data for a specific clinic, you can simply export that clinic’s database.
Database-per-tenant isolation also enables per-clinic customization. Each database can have a slightly different schema to accommodate clinic-specific fields or workflows. You can even run different software versions for different clinics during major migrations, reducing risk.
The operational challenges are significant. Managing hundreds or thousands of databases requires sophisticated automation. Schema migrations must be orchestrated across all tenant databases. Backup and disaster recovery complexity multiplies. Cross-tenant analytics becomes difficult — you can’t simply query across databases to generate platform-wide metrics.
Cost efficiency suffers at scale. Each database instance consumes resources even when idle. Cloud database services charge per instance, making this model expensive beyond a certain customer count.
This model works well for large enterprise customers willing to pay premium prices for maximum isolation, or for highly regulated scenarios where the compliance benefits justify the operational complexity. It’s common in healthcare SaaS serving hospital networks where each hospital expects dedicated infrastructure.
Schema-Per-Tenant Isolation
A middle ground uses a single database instance with separate schemas (or table prefixes) for each tenant. Tenant A’s data lives in tables like tenant_a_patients, tenant_a_appointments, while Tenant B uses tenant_b_patients, tenant_b_appointments.
This reduces infrastructure overhead while maintaining clear data separation. All tenants share database compute resources, improving efficiency. Schema migrations are simpler — apply once to the database, affecting all tenant schemas. Cross-tenant queries for analytics are possible but require careful access control.
Security relies on application-layer enforcement. Your code must consistently prefix all queries with the correct tenant identifier. A bug that fails to add the tenant filter could leak data across clinics. This requires rigorous code review, automated testing, and possibly query-level access controls.
The schema-per-tenant model suits platforms with moderate-sized clinics (dozens to hundreds of users each) where isolation is important but dedicated infrastructure isn’t economically viable. It provides a clearer compliance story than row-level isolation while avoiding the operational burden of a database per tenant.
Row-Level Tenant Isolation
The most efficient multi-tenant model uses shared tables with a tenant ID column. All clinics’ data lives in the same tables, separated by a clinic_id, and every query filters by tenant.
This approach maximizes efficiency: shared infrastructure, simple schema migrations, and easy cross-tenant analytics — making it cost-effective for small clinics.
However, security relies on strict query filtering. A missing tenant condition can expose all data. Strong defense-in-depth is essential: enforced database views, middleware-level tenant scoping, thorough testing, and runtime safeguards.
Row-level isolation works best for platforms serving many small clinics where cost efficiency outweighs the need for dedicated infrastructure.
Hybrid Models for Different Customer Tiers
Sophisticated platforms use hybrid isolation models, offering different tiers for different customer segments. Enterprise hospital networks get database-per-tenant isolation. Mid-market clinic groups get schema-per-tenant. Small independent practices share row-level isolated infrastructure.
This requires architectural complexity — your platform must support multiple deployment models. But it enables serving different market segments profitably while meeting diverse security and compliance requirements.
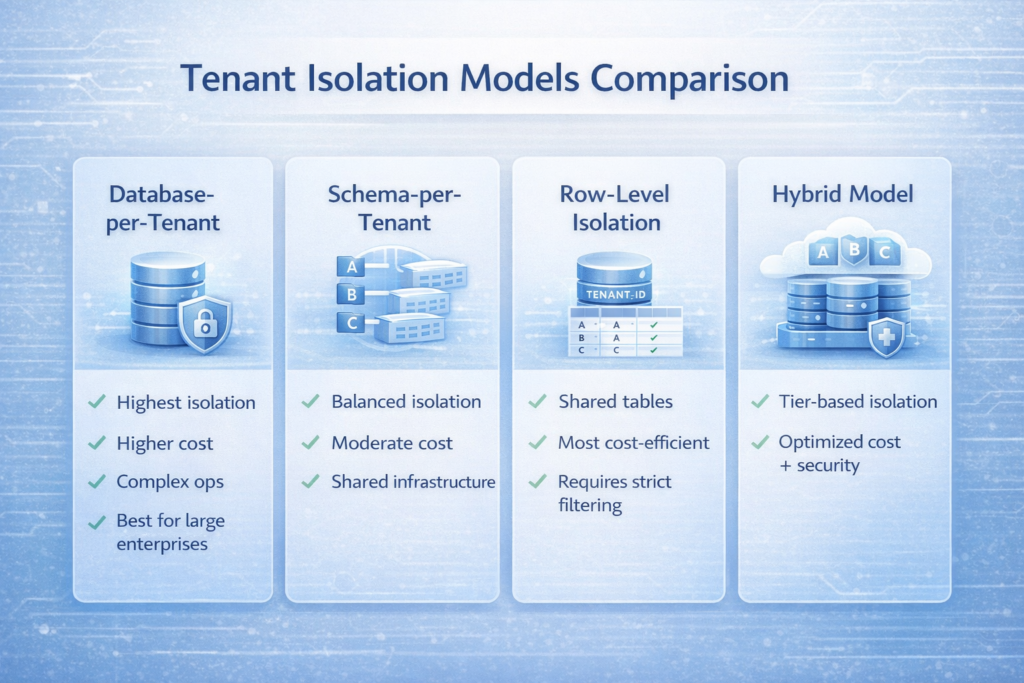
| Isolation Model | Security Strength | Cost Efficiency | Operational Complexity | Best For |
| Database-per-tenant | Highest | Low | High | Large enterprises, maximum compliance requirements |
| Schema-per-tenant | Medium-High | Medium | Medium | Mid-market clinics, balanced approach |
| Row-level | Medium | Highest | Low | Small practices, high customer count |
| Hybrid | Variable | Optimized | Highest | Multi-tier SaaS serving diverse segments |
Multi-Region Compliance: Navigating Geographic Complexity
Healthcare data residency requirements vary dramatically across jurisdictions. HIPAA governs US healthcare data. GDPR affects European Union operations. Canada’s PIPEDA has specific requirements. Many countries prohibit storing citizens’ health data outside national borders.
Data Residency Architecture
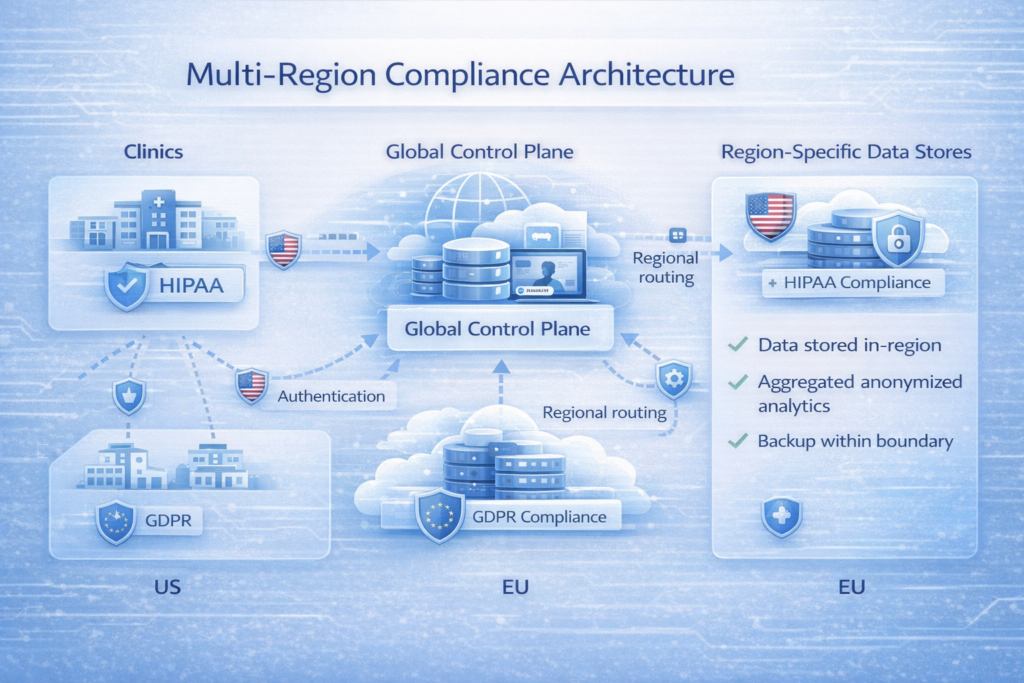
True multi-region compliance requires data residency — ensuring patient data physically resides in the required jurisdiction. This means deploying infrastructure in multiple geographic regions and routing data to the appropriate region based on patient or clinic location.
The architectural pattern involves regional data stores with centralized control planes. Patient data, clinical records, and other PHI live in region-specific databases. Metadata about clinics, users, and configurations can live centrally or be replicated across regions.
When a clinician in Germany accesses patient records, the request routes to the EU infrastructure. A California-based clinic accesses US-based infrastructure. Your application must determine the correct region for each request and route accordingly.
This requires sophisticated request routing. Typically, a clinic configuration includes a data_region attribute. User authentication determines which clinic they belong to, which determines the data region. All subsequent requests in that session route to the appropriate regional infrastructure.
Cross-Region Challenges
Multi-region architectures create operational complexity. Code deployments must be orchestrated across regions. Database schema changes must be synchronized. Monitoring, logging, and alerting need region-specific configurations while rolling up to central dashboards.
Disaster recovery becomes more complex. If EU infrastructure fails, US infrastructure can’t simply take over — it doesn’t contain EU patient data. You need region-specific failover strategies, typically involving backup regions within the same compliance boundary (e.g., EU-West failover to EU-Central).
Analytics and reporting span regions. Generating platform-wide metrics requires aggregating data from multiple regional stores without violating data residency requirements. This typically means running analytics within each region, then aggregating anonymized results centrally.
Compliance Documentation
Multi-region compliance isn’t just technical — it’s documentary. You need clear documentation of data flows, processing locations, and compliance controls for each jurisdiction. Enterprise customers will audit this during procurement.
This includes data processing agreements for each jurisdiction, certifications (HITRUST, SOC 2, ISO 27001) scoped to specific regions, and clear breach notification procedures meeting local requirements. Many platforms maintain jurisdiction-specific compliance documentation sets, tailored to local regulatory language.
Enterprise IAM Integration: SSO and Beyond
Enterprise healthcare organizations don’t want another password to manage. They expect your platform to integrate with their existing Identity and Access Management systems, inherit their security policies, and support their user lifecycle management.
SAML and OpenID Connect Integration
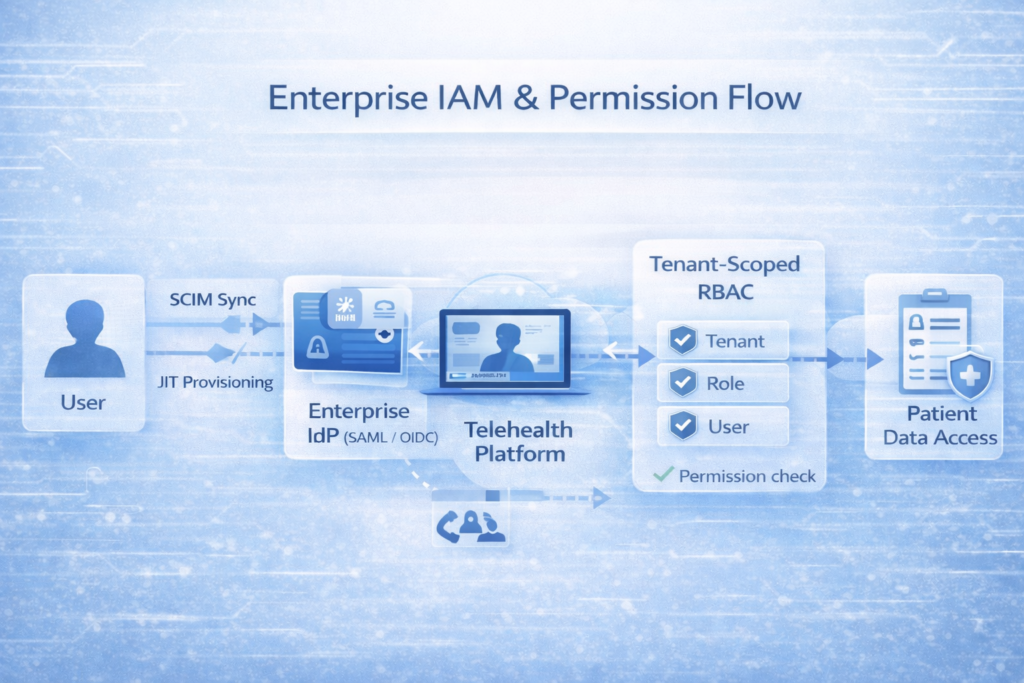
The foundation is supporting industry-standard authentication protocols — SAML 2.0 and OpenID Connect (OIDC). These allow your platform to delegate authentication to the customer’s Identity Provider (IdP), like Okta, Azure AD, or Google Workspace.
Implementation requires a multi-tenant SSO configuration system. Each clinic can configure its own IdP connection. When a user from Clinic A logs in, your platform redirects them to Clinic A’s IdP. After authentication, the IdP redirects back with assertions about the user’s identity and potentially their roles or group memberships.
Your platform must map IdP-provided attributes to your internal user model. If Azure AD sends a user with group membership Physicians, your system might map that to internal roles as a provider with specific permissions. This mapping must be configurable per clinic — different organizations’ structures their directories differently.
Just-In-Time Provisioning
Enterprise customers want automatic user provisioning. When they add someone to their directory, that person should automatically get access to your platform with appropriate permissions. When they’re removed, access should be immediately revoked.
Just-in-time (JIT) provisioning creates user accounts automatically during the first login. When a new physician authenticates via SSO, your platform creates their user record with roles derived from IdP attributes. This eliminates manual user management and ensures access follows HR processes.
SCIM (System for Cross-domain Identity Management) provides more sophisticated provisioning. It’s an API standard allowing IdPs to push user lifecycle events to your platform. When an employee is hired, the IdP creates them in all connected systems. When terminated, the IdP deactivates all its accounts.
Implementing SCIM means exposing endpoints for user creation, update, and deletion. The IdP authenticates using OAuth 2.0 and sends JSON payloads describing user changes. Your platform processes these events, creating, updating, or disabling user accounts.
Role-Based Access Control at Scale
Enterprise telehealth requires granular permissions. Physicians access and update clinical records. Nurses document vitals but don’t prescribe. Admin staff schedule visits without seeing clinical data. Clinic admins configure workflows without accessing patient information.
In multi-tenant systems, RBAC must be tenant-scoped — being a “Physician” in Clinic A grants no access in Clinic B.
Advanced platforms use hierarchical RBAC: base roles define standard permissions, clinics can customize or create roles, and individual users can receive additional scoped permissions when needed.
Permission checks must consider both the user’s role and the tenant context. Before showing patient data, verify: Does this user belong to this clinic? Does their role allow viewing patient data? Does this specific patient belong to this clinic? All three checks must pass.
Feature Toggles and Clinic-Specific Customization
Not every clinic needs every feature. Some want advanced analytics, others don’t. Certain features may only be relevant to specific specialties. Allowing customization without fragmenting your codebase requires feature flag architecture.
Feature Flag Infrastructure
Feature flags (or feature toggles) are configuration controls that enable or disable functionality. They decouple deployment from release — you can deploy code for a new feature but keep it disabled until ready, then enable it for specific customers.
In multi-tenant platforms, feature flags operate at multiple scopes:
Global flags control features across the entire platform. These gates major new capabilities during phased rollouts or provide kill switches for problematic features.
Tenant-level flags allow per-clinic customization — Clinic A enables advanced scheduling, Clinic B doesn’t; one enterprise customer receives beta analytics, others don’t.
User-level flags add finer control, granting specific individuals beta access or tailored capabilities.
Implementation typically relies on a feature flag service (e.g., LaunchDarkly, Split.io, or custom-built) that evaluates flags at runtime. Before rendering UI or executing logic, the system checks whether the feature is enabled for the current tenant, user, or region.
Configuration Management Beyond Features
Feature flags handle binary on/off decisions. Many customizations require configuration values — maximum appointment duration, available appointment types, required patient intake fields, or integrated third-party services.
Sophisticated platforms provide hierarchical configuration management. Default values apply globally. Tenant-specific configurations override defaults for specific clinics. Some platforms even allow clinic administrators to expose certain configurations to individual providers.
This requires a flexible configuration schema that can accommodate diverse needs without becoming unmaintainable. Common approaches include:
Typed configuration objects, where each feature defines its configuration structure. The scheduling feature might have a SchedulingConfig object with properties for duration increments, buffer times, and overbooking rules.
Key-value stores with namespaces allowing arbitrary configuration keys organized hierarchically. scheduling.default_duration might be 30 globally, overridden to 45 for a specific clinic.
Feature-specific settings pages in the admin interface where clinic administrators configure enabled features. This requires building a flexible UI that adapts to which features are enabled and what configuration they require.
Managing Configuration Complexity
As platforms grow, configuration complexity can become overwhelming. Hundreds of flags and thousands of configuration values create an operational burden and increase bug risk. Strategies for managing this include:
Configuration versioning and audit trails tracking who changed what configuration when. This is essential for debugging issues and supporting compliance audits.
Configuration validation ensures values meet constraints. If the minimum appointment duration is 15 minutes, the system should prevent configuring 10 minutes.
Configuration inheritance visualization showing which settings come from global defaults versus tenant-specific overrides. This helps clinic administrators understand effective configurations.
Scheduled flag retirement forces teams to either promote flags to permanent settings or remove them. Flags intended for short-term rollouts shouldn’t live forever.
Central Analytics vs. Local Autonomy
Enterprise customers want visibility into their operations. But they also value autonomy and privacy. Platform operators need aggregate metrics for product decisions. This creates tension between centralized analytics and tenant privacy.
Centralized Analytics Platform
A centralized analytics platform aggregates data across all clinics, providing platform-wide insights. This enables understanding overall product usage, identifying performance bottlenecks, and making data-driven product decisions.
The architecture typically involves event streaming from regional application servers to a central analytics data warehouse. User actions, clinical workflows, and system events become structured events streamed to the analytics infrastructure.
Privacy and compliance require careful handling. PHI must be stripped or tokenized before events leave the regional infrastructure. A “patient_viewed” event might include the clinic ID, provider role, and patient age bracket — but not the patient’s name or medical record number.
Aggregated analytics provide value without exposing individual patient data. You can measure average appointment duration across the platform, most common appointment types, feature adoption rates by clinic size, and performance metrics by region.
Clinic-Level Analytics and Reporting
Clinics require tenant-level analytics — utilization, revenue, satisfaction, provider productivity, and outcomes — delivered with greater detail than platform-wide metrics and fully isolated per tenant.
Architecture typically includes clinic-specific dashboards powered by their own data stores, ensuring each clinic accesses only its data, including patient-level detail (governed by role-based controls).
Advanced platforms enable customizable reporting, allowing administrators to build dashboards, define metrics, and schedule reports — via embedded BI tools or flexible reporting infrastructure.
Anonymized Data Sharing
Some platforms allow clinics to opt into anonymized data sharing for research or benchmarking — for example, comparing their no-show rate against aggregated peers. This delivers insight without compromising privacy.
Proper implementation requires strong anonymization: cohort-level aggregation to prevent re-identification, plus techniques like k-anonymity and differential privacy. Participation must be explicit, with clear documentation on what data is shared, how it’s protected, and what value clinics receive in return.
Performance and Scalability Patterns
Multi-tenant architectures must scale efficiently. Serving 1,000 clinics with 10,000 total providers requires different strategies than serving 10 clinics with 100 providers.
Resource Pooling and Isolation
Shared infrastructure enables cost efficiency but creates contention risk. One clinic’s usage spike shouldn’t degrade performance for others. This requires resource pooling with quality-of-service guarantees.
Database connection pooling with per-tenant limits prevents one clinic from exhausting connections. API rate limiting with tenant-aware quotas prevents abuse. Background job processing with tenant-aware queuing prevents one clinic’s batch jobs from starving others.
For enterprise customers on premium tiers, consider dedicated resource pools. Their database queries run on reserved capacity. Their API calls bypass standard rate limits. Their batch jobs get priority queue processing.
Caching Strategies
Effective caching dramatically improves multi-tenant platform performance. But naive caching can leak data across tenants. Cache keys must include tenant identifiers. A query for “upcoming appointments” must be cached separately for each clinic.
Multi-layer caching strategies optimize different access patterns:
Application-level caching stores frequently accessed data in-memory within application servers. User sessions, clinic configurations, and feature flags are good candidates.
Distributed caching with Redis or Memcached provides shared caching across application servers. This works well for data that’s expensive to compute but accessed frequently across instances.
CDN caching serves static assets and even dynamic content for geographically distributed clinics. A clinic in California gets assets from US edge nodes; one in Germany from EU nodes.
Database Optimization
Multi-tenant databases face unique optimization challenges. Queries span multiple tenants. Indexes must support both tenant-specific and cross-tenant queries. Query planners must optimize for varied data distributions.
Tenant-aware indexing creates indexes that include tenant identifiers. A query for WHERE clinic_id = ? AND appointment_date > ? benefits from an index on (clinic_id, appointment_date).
Partition pruning distributes data across physical partitions by tenant or date range. Queries touching only specific tenants access only relevant partitions, reducing I/O.
Query optimization requires monitoring for slow queries and understanding their tenant distribution. A query that’s fast for most clinics but slow for your largest customer needs special attention.
Building for Enterprise: Lessons and Partnership
Scaling a telehealth platform from a single clinic to a multi-tenant enterprise system requires deliberate architecture, iterative evolution, and deep healthcare expertise.
At Trembit, we’ve designed and scaled platforms across markets and regulatory environments — balancing standardization with flexibility, security with usability, and operational efficiency with customer autonomy.
Our approach starts with understanding your current architecture and growth trajectory. Are you serving 10 clinics planning to reach 100, or 100 planning to reach 1,000? Are you expanding internationally? Are you moving upmarket to enterprise customers? Each growth vector requires different architectural priorities.
We implement these patterns in practice — designing tenant isolation aligned to your customer mix, multi-region compliance architectures for diverse regulatory environments, enterprise IAM integrations for complex org structures, and feature flag frameworks that enable customization without fragmenting your codebase.
Beyond initial architecture, we provide ongoing support for operational maturity. This includes monitoring and observability frameworks for multi-tenant systems, incident response procedures that isolate tenant-specific issues, and disaster recovery strategies that respect data residency requirements.
The Road to Enterprise Maturity
Building enterprise-grade telehealth infrastructure is a continuous journey, not a destination. The architecture that serves 50 clinics well may need refinement at 500. International expansion introduces new compliance requirements. Moving upmarket brings customers with sophisticated integration requirements.
Successful platforms evolve through careful planning and measurement. Instrument your systems to understand tenant-specific usage patterns, performance characteristics, and cost drivers. Use this data to inform architectural decisions. Maybe most clinics are small enough for row-level isolation, but your fastest-growing customer needs dedicated infrastructure. Most traffic is domestic, but international expansion requires regional infrastructure investment.
The platforms that thrive in competitive healthcare SaaS markets combine strong technical foundations with operational excellence. They make it easy for enterprise customers to integrate, secure for patients to trust, and efficient for operators to scale profitably. They achieve this through thoughtful architecture, careful implementation, and partnership with teams who understand both healthcare technology and enterprise requirements.
The future of healthcare is multi-tenant, distributed, and compliant by design. Building platforms ready for this future requires balancing competing concerns — security and performance, customization and maintainability, autonomy and control. With the right architecture and experienced partners, these tensions become strengths rather than constraints.