Video infrastructure is one of the most consequential technology decisions a telemedicine CTO makes — and one of the most frequently regretted.
The teams that regret it fall into two camps. The first bought a third-party video SDK, scaled to the point where vendor constraints became product constraints, and found themselves locked into a platform that couldn’t support their compliance requirements or differentiated features. The second was built from scratch, underestimated WebRTC complexity, burned 18 months of engineering capacity, and ended up with a fragile system that two engineers are afraid to touch.
Both regrets are avoidable. The decision isn’t inherently hard — it’s hard when it’s made without a clear framework, or when it’s made too early before the right constraints are visible.
This article gives CTOs a structured way to think through the choice across five dimensions: compliance, cost, control, capability, and time-to-market. At the end is a decision matrix you can adapt to your specific situation.
Why Telemedicine Is a Special Case
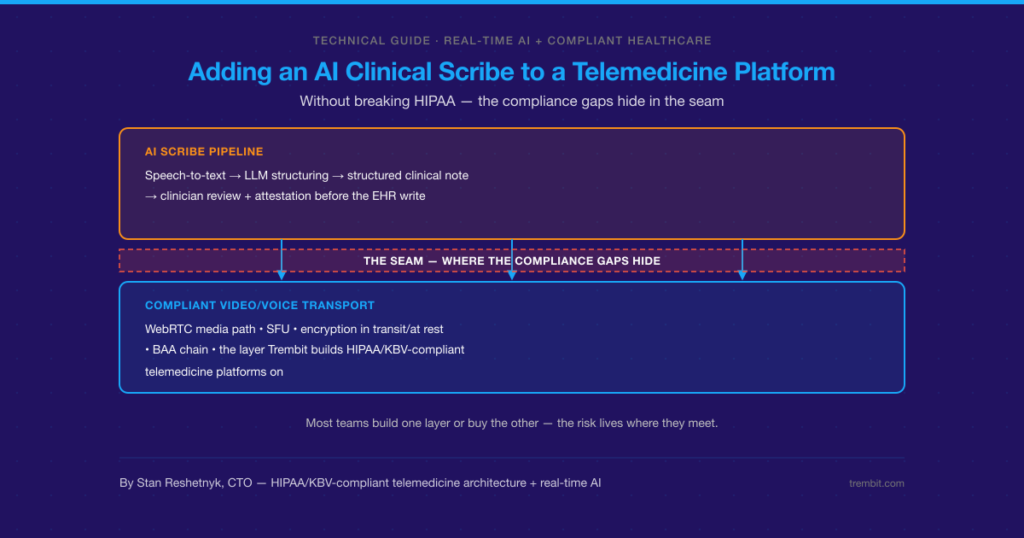
Before getting into the framework, it’s worth acknowledging that telemedicine video infrastructure isn’t generic video calling. The differences compound at every layer of the stack.
Regulatory requirements are specific and jurisdiction-dependent. In Germany, KBV Anlage 31b mandates particular encryption, data residency, and audit logging requirements. In the US, HIPAA requires Business Associate Agreements with every infrastructure subprocessor. In France, the HDS certification framework applies. A general-purpose video SDK that hasn’t been built for healthcare may leave you responsible for compliance gaps that the vendor has no incentive to close.
Clinical context changes quality requirements. A dropped frame during a casual video call is annoying. A dropped frame during auscultation guidance, wound assessment, or a psychiatric crisis is a clinical risk. The reliability bar is genuinely different.
The patient and practitioner experience is your product. Unlike internal tooling, where “good enough” is acceptable, the video experience in telemedicine directly affects patient outcomes, practitioner adoption, and reimbursement eligibility. Corners cut on infrastructure show up in churn and in clinical trust.
With that context, here’s the framework.
Dimension 1: Compliance Footprint
This is the first filter, not the last. Before evaluating features or cost, map your compliance obligations and check whether each option can satisfy them without heroic custom engineering.
Questions to ask:
- Does your target market require specific certifications (KBV, HIPAA, HDS, GDPR, etc.)?
- Which of those certifications require data residency in specific regions?
- Can the vendor provide a Business Associate Agreement or Data Processing Agreement?
- Where are the vendor’s media servers physically located — and can you pin to compliant regions?
- Does the vendor’s architecture allow or require server-side media access (which may break E2E encryption requirements)?
Build gives you full control over compliance architecture, but requires you to build and maintain compliance evidence yourself. This is viable but expensive.
Buy depends entirely on the vendor. Some (Daily.co, Whereby for Business, Vonage/Video API) have invested heavily in HIPAA compliance. Fewer have navigated European healthcare certifications. Read the DPA and BAA carefully — “HIPAA compliant” on a landing page is not the same as a signed BAA with the right subprocessor disclosures.
Partnering with a specialized engineering team means compliance architecture is built into the engagement from day one, with a partner who has done it before and can navigate certification processes alongside you.
Dimension 2: Total Cost of Ownership
Build vs. buy cost analyses are almost always wrong in the same direction: they undercount the cost of building and overcount the cost of buying. Here’s a more complete picture.
True cost of building:
- Senior WebRTC engineers are specialized and expensive — $180K–$280K+ annually in most markets
- Initial build timeline for a production-grade system: 9–18 months for a small team
- Ongoing maintenance: WebRTC browser APIs change; Safari alone has broken multiple implementations per year
- TURN server infrastructure, media processing, and scaling infrastructure all carry ongoing costs
- Internal knowledge concentration risk: when the one engineer who understands the SFU leaves, you have a problem
True cost of buying:
- Per-minute or per-participant pricing looks cheap in pilots and scales uncomfortably at volume.
- At 100,000 consultation-minutes per month, vendor costs can reach $10K–$30K/month, depending on the provider.
- Feature limitations that require workarounds add hidden engineering cost.
- Vendor lock-in creates leverage risk at contract renewal.
- Migration costs if you need to switch are high.
True cost of partnering:
- Engagement cost is front-loaded but bounded.
- You own the resulting codebase — no ongoing per-minute charges.
- Specialized partners bring relevant experience, compressing the timeline.
- Ongoing support retainer is optional, not mandatory.
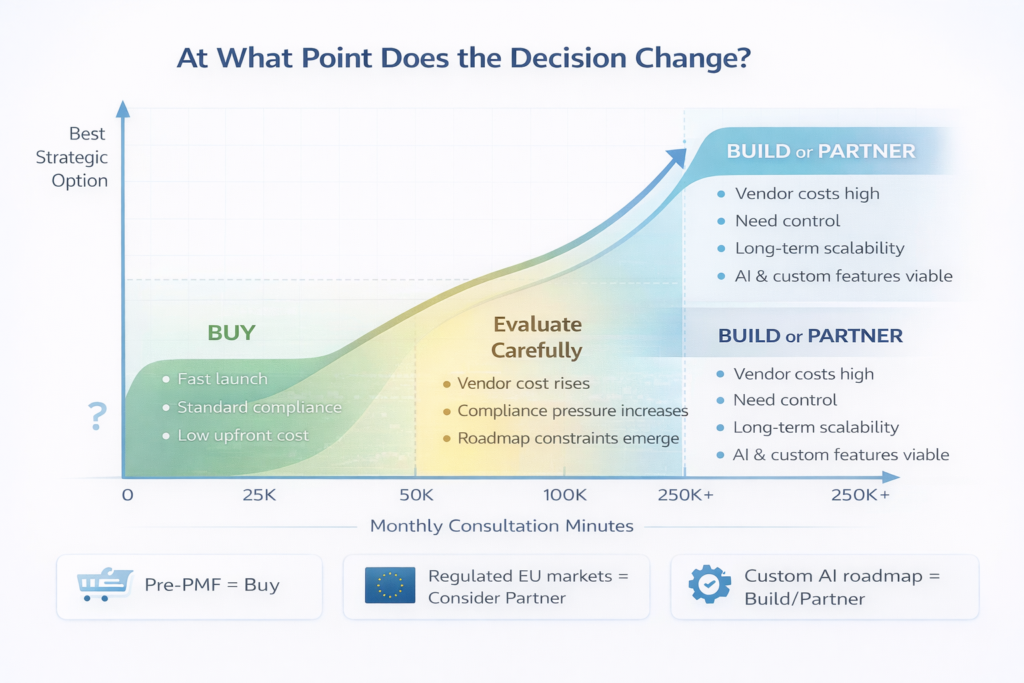
The crossover point where building (or partnering to build) becomes cheaper than buying is typically around 50,000–100,000 consultation-minutes per month, depending on your vendor’s pricing tier. Below that threshold, buy. Above it, the math shifts.
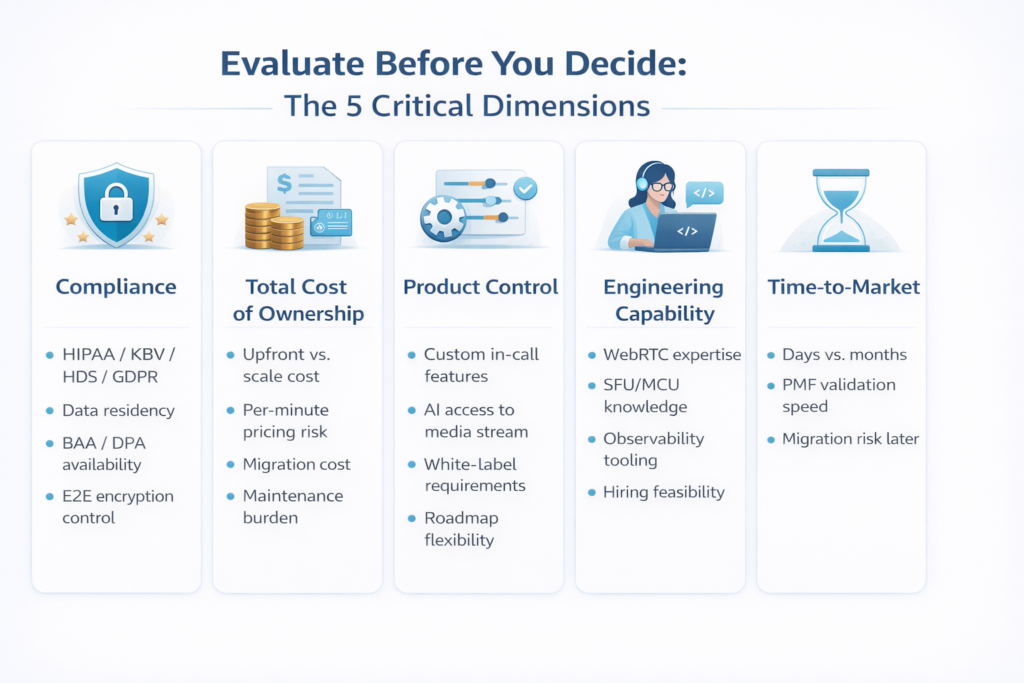
Dimension 3: Product Control Requirements
The right answer here depends on how differentiated your video experience needs to be.
Buy is sufficient if:
- Your video feature is a standard one-to-one or small-group consultation.
- You don’t need custom in-call features (e.g., integrated clinical forms, annotation tools, custom recording pipelines)
- Your compliance requirements match what the vendor already supports.
- You’re pre-product-market-fit, and video is table stakes, not a differentiator.
Building or partnering is necessary if:
- You need features that the vendor doesn’t support and won’t prioritize
- Compliance requirements exceed what the vendor infrastructure can satisfy.
- You need white-label infrastructure with no third-party domains in network requests.
- Your roadmap includes AI-powered features (transcription, real-time translation, clinical decision support) that require access to the media stream.
- You’re building for a regulated market with specific certification requirements that the vendor hasn’t pursued.
The question to ask is: In 18 months, will vendor constraints limit our product roadmap? If you can’t answer confidently, assume yes.
Dimension 4: Internal Engineering Capability
Honest capability assessment is where many build decisions go wrong. WebRTC is not general-purpose backend or frontend engineering. It requires specific expertise in:
- Network protocols (ICE, STUN, TURN, DTLS, SRTP)
- Media encoding and adaptive bitrate algorithms
- Browser API differences and regression patterns
- SFU/MCU architecture and media server tuning
- Observability for real-time media systems
Before deciding to build, answer these questions:
- Do you have engineers with production WebRTC experience, or will they be learning on the job?
- Can you hire the specialized talent needed, and how long will that take?
- Is video infrastructure a core competency you want to develop internally, or a capability you want to acquire?
- What’s the opportunity cost of senior engineering time spent on infrastructure vs. clinical product features?
Building from scratch without relevant experience is the most common source of the failing WebRTC codebases we inherit. The decision to build isn’t wrong — the decision to build without acknowledging the capability gap is.
Dimension 5: Time-to-Market Pressure
This dimension is often decisive for early-stage platforms. A vendor SDK can get you to a working demo in days and a production feature in weeks. A custom build takes months at a minimum.
The nuance is that time-to-market pressure is temporary, and compliance requirements are permanent. Teams that buy to move fast, then discover the vendor can’t satisfy their compliance requirements, face a more painful migration than if they’d made the right foundational choice earlier.
A pragmatic path that works: use a vendor SDK to validate product-market fit and clinical workflow, then partner to build a compliant, owned infrastructure as you scale. This preserves early velocity while avoiding the permanent costs of the wrong vendor dependency.
The Decision Matrix
| Build In-House | Buy (Vendor SDK) | Partner to Build | |
| Compliance control | Full | Vendor-dependent | Full |
| Upfront cost | High | Low | Medium |
| Cost at scale | Low | High | Low |
| Time to first call | 6–18 months | Days–weeks | 3–6 months |
| Feature flexibility | Full | Constrained | Full |
| Internal knowledge req. | Very high | Low | Medium |
| Vendor lock-in risk | None | High | None |
| Best for | Large teams, clear roadmap | Pre-PMF, standard use case | Scaling teams, regulated markets |
A Note on the “Partner” Path
Partnering is underused as an option because it’s less visible than “build vs. buy.” But for telemedicine platforms in particular, it deserves serious consideration.
A specialized engineering partner brings what internal teams typically lack when they decide to build: production WebRTC experience, compliance architecture knowledge, and the ability to compress a 12-month learning curve into a 3–4 month engagement. You get a codebase you own, infrastructure you control, and a team that can hand off cleanly to your engineers.
The key is choosing a partner with genuine depth in both real-time media systems and healthcare compliance — not a generalist agency that has done one WebRTC project.
Trembit works with telemedicine platforms across exactly this decision point. Whether you’re evaluating options, migrating off a vendor you’ve outgrown, or rescuing a struggling in-house build, we help teams make the right architectural choices for regulated, high-reliability video infrastructure. We’ve navigated HIPAA, KBV, and GDPR requirements in production systems, and we can help you build something that scales without becoming a liability.
Start with a technical conversation — no commitment, just clarity on where you stand.
The Decision in One Sentence
Buy if you’re pre-scale and compliance requirements are standard. Build (or partner to build) if you’re scaling, your compliance requirements are specific, or your product roadmap requires control that your vendor won’t give you.
The framework is a tool for pressure-testing your assumptions — not a substitute for them. The teams that make this decision well are the ones who know which constraints are real, which are imagined, and which will matter in two years even if they don’t today.