Virtual reality has been described as the future of medicine for nearly a decade. The pitches are compelling: immersive surgical simulations, VR-assisted pain management, remote consultations so lifelike they rival an in-person visit. The reality, as with most emerging technology in healthcare, is more nuanced.
VR is not the future of telemedicine. In specific, well-defined use cases, it is the present — deployed, clinically validated, and producing measurable outcomes. In others, it remains experimental or economically impractical. The challenge for healthcare technology leaders is knowing the difference.
This article takes a clear-eyed look at where VR in telemedicine is delivering real value today, what the evidence actually says, and what organizations need to consider before investing.
Why VR and Telemedicine Are a Natural Pairing — in Theory
Standard video telemedicine is fundamentally limited by its two-dimensionality. A clinician on a screen can ask questions, observe behavior, and review shared documents or imaging. What they cannot do is simulate physical presence, create an immersive therapeutic environment, or give a patient a sense of being somewhere other than their own home.
VR addresses precisely these gaps. A headset can place a patient in a calm, controlled virtual environment. It can simulate clinical scenarios for training. It can guide a patient through a rehabilitation exercise with real-time visual feedback. It can allow a specialist to examine a three-dimensional model of a patient’s anatomy built from their imaging data — remotely, collaboratively, in real time.
The question is not whether these capabilities are technically impressive. They are. The question is whether they are clinically useful, accessible, and economically viable at scale.
Where VR in Telemedicine Actually Works Today
1. Mental Health and Anxiety Treatment
This is, without question, the most clinically mature application of VR in telemedicine today. The evidence base for VR-delivered exposure therapy — the gold-standard treatment for phobias, PTSD, and certain anxiety disorders — is robust and growing.
VR exposure therapy (VRET) allows clinicians to deliver controlled, graded exposure to feared stimuli without the logistical complexity of real-world scenarios. A veteran with combat-related PTSD can be exposed to contextually accurate but controllable environments. A patient with a fear of heights can practice standing on a virtual ledge. A patient with social anxiety can rehearse interactions in progressively challenging virtual settings.
Critically, these sessions can be conducted remotely. The patient wears a headset at home; the clinician monitors and adjusts the session via a connected interface. Studies published in peer-reviewed journals, including JMIR Mental Health and Frontiers in Psychiatry, have demonstrated outcomes comparable to in-person exposure therapy for several conditions.
What makes this work:
- The therapeutic mechanism (exposure) maps naturally onto what VR does well.
- Sessions do not require physical examination or complex hardware beyond the headset.
- Remote delivery expands access to evidence-based therapy in underserved areas.
- Platforms like Oxford VR, Psious, and XRHealth have built clinically validated commercial products in this space.
2. Pain Management
VR-based pain distraction has moved well beyond proof-of-concept. The underlying mechanism — immersive VR reduces perceived pain by competing for attentional and cognitive resources — is well established in the literature. Notably, Hoffman et al. demonstrated meaningful pain reduction during burn wound care using VR as early as the mid-2000s, and subsequent research has confirmed the effect across multiple contexts.
In a telemedicine context, VR pain management has found a specific niche in chronic pain programs. Patients managing conditions such as fibromyalgia, chronic back pain, or pain following injury can use guided VR experiences prescribed and monitored remotely by pain specialists. The content — typically calming, immersive environments combined with guided mindfulness or breathing exercises — is delivered via consumer-grade headsets such as the Meta Quest.
AppliedVR (now EaseVRx, FDA-authorized) offers a clinically validated remote program for chronic lower back pain. Patients receive a headset and structured daily VR sessions, monitored and adjusted by their care team. This is not speculative — it is a commercially available, FDA-cleared product.
3. Physical Rehabilitation and Motor Recovery
Remote physical rehabilitation is one of the most promising current applications of VR in telemedicine, particularly for stroke recovery and musculoskeletal rehabilitation.
Traditional telehealth rehabilitation is constrained by the same limitations as video consultations generally: the clinician can watch but cannot easily guide, measure, or correct movement. VR changes this. A rehabilitation platform can track patient movement via the headset’s built-in sensors and controllers, provide real-time visual feedback, gamify exercises to improve adherence, and transmit session data to the supervising therapist.
Platforms like MindMaze, XRHealth, and Penumbra’s REAL System are deployed in clinical settings for post-stroke motor rehabilitation. Remote delivery of these programs allows patients to continue structured rehabilitation at home between clinical visits — addressing one of the most persistent problems in stroke recovery, which is the gap between discharge and adequate rehabilitation volume.
The evidence here is promising but still maturing. Studies show improvements in upper limb function, patient engagement, and adherence compared to conventional home exercise programs. Large-scale randomized controlled trials comparing remote VR rehabilitation to standard care are ongoing.
4. Surgical Planning and Remote Collaboration
This application sits at the intersection of VR and telemedicine in a more specialized clinical context. Using patient imaging data (CT, MRI) converted into three-dimensional VR models, surgeons can collaboratively review complex anatomy remotely — planning procedures, discussing approaches, and training residents without being in the same room.
Companies such as Surgical Theater and Medivis have built platforms that enable this workflow. A neurosurgeon consulting on a complex case from a different institution can explore a patient-specific 3D model of the relevant anatomy in VR alongside the operating surgeon, with both participants present in the same virtual space.
This is not telemedicine in the conventional sense, but it is a genuine and currently deployed use of VR that extends the reach of specialist expertise — one of telemedicine’s core value propositions.
5. Medical Education and Remote Clinical Training
Healthcare professional training has adopted VR at a meaningful scale. This use case is important in a telemedicine context because it addresses one of telemedicine’s infrastructure problems: clinicians who are not adequately trained for remote clinical assessments perform them less effectively.
VR simulation platforms allow trainees to practice clinical examinations, emergency scenarios, and communication skills in realistic environments — remotely and repeatedly. Osso VR and Fundamental Surgery are deployed across medical schools and hospital systems. The evidence for VR surgical training specifically shows skill transfer to the operating room, with some studies showing meaningful improvement in operative performance.
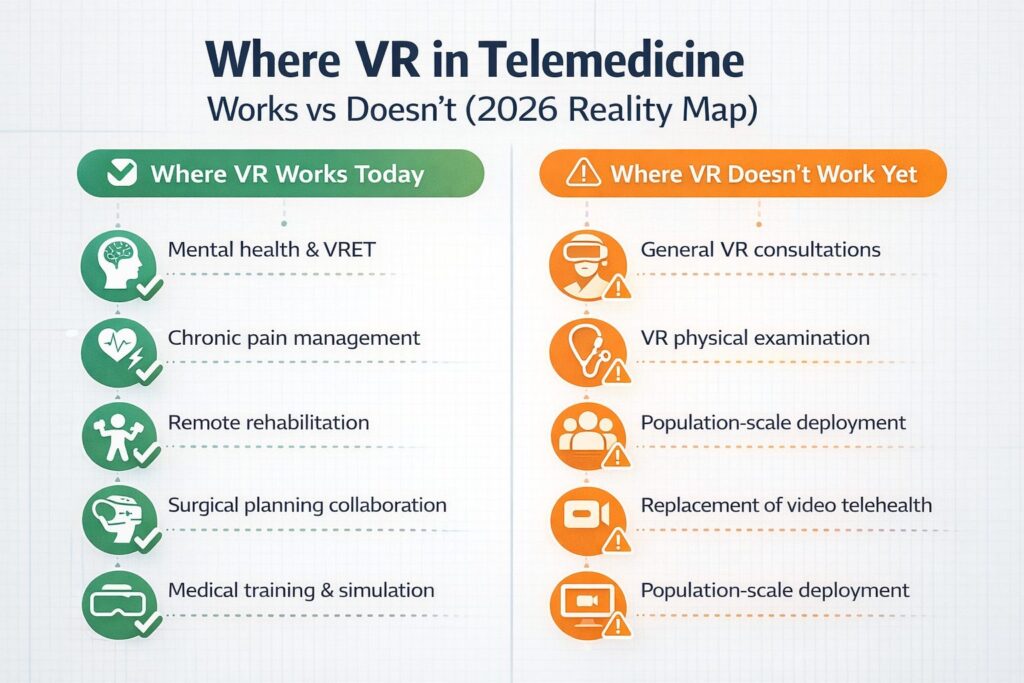
What Does Not Work Yet (But Gets Oversold)
Clarity about where VR works requires equal clarity about where it does not — at least not yet, not at scale.
General remote consultation via VR remains impractical for most telehealth interactions. The hardware cost, setup complexity, and lack of clear clinical benefit over video make it a poor replacement for standard video consultations in routine primary or specialty care. The use cases that work are specific; the general case does not.
VR physical examination is a persistent research aspiration but not a clinical reality. The absence of haptic feedback with sufficient fidelity means that palpation, auscultation, and other examination modalities cannot be replicated meaningfully in VR with current hardware. This limits the framework’s utility in diagnostic contexts that depend on physical examination.
Population-scale deployment faces real barriers. Consumer VR headsets are more accessible than they were five years ago, but a significant portion of the patient population — elderly patients, those with low digital literacy, or those in areas without reliable broadband — cannot realistically use them.
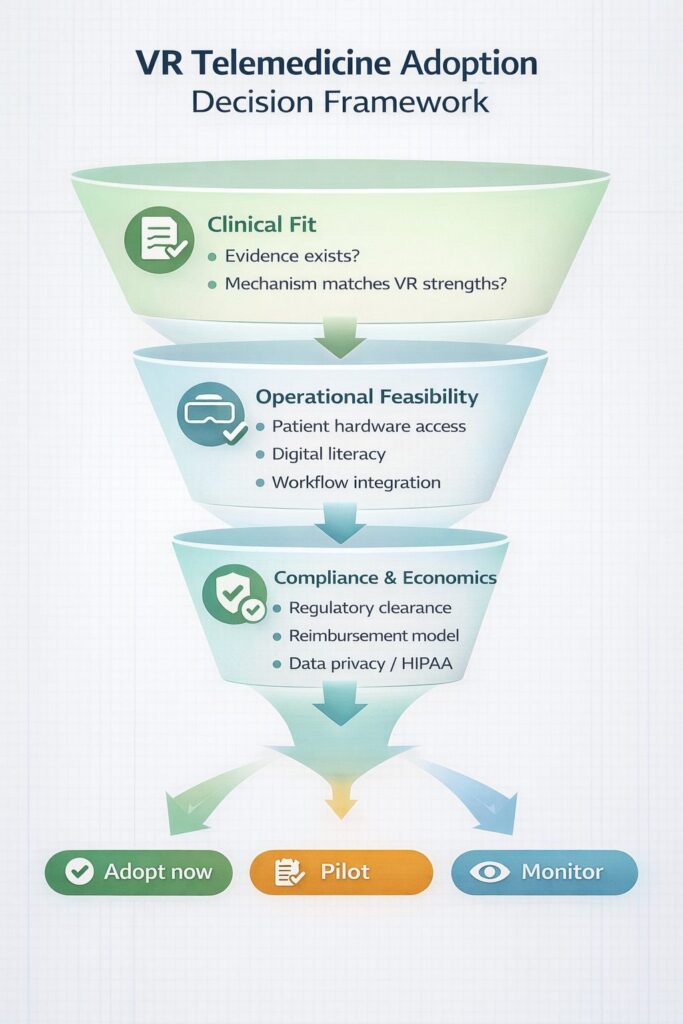
Key Considerations Before Investing
| Consideration | What to Evaluate |
| Clinical evidence | Is there peer-reviewed evidence for this specific application, or is the ROI claim extrapolated from adjacent research? |
| Regulatory status | Is the VR solution FDA-cleared or CE-marked for clinical use, or is it a wellness product? |
| Hardware access | Can your target patient population realistically acquire and use the required headset? |
| Reimbursement | Does your payer mix cover VR-delivered telehealth services for this indication? |
| Integration | Does the platform integrate with your EHR and existing telehealth infrastructure? |
| Data privacy | Does the solution meet HIPAA requirements? VR platforms collect substantial behavioral and biometric data. |
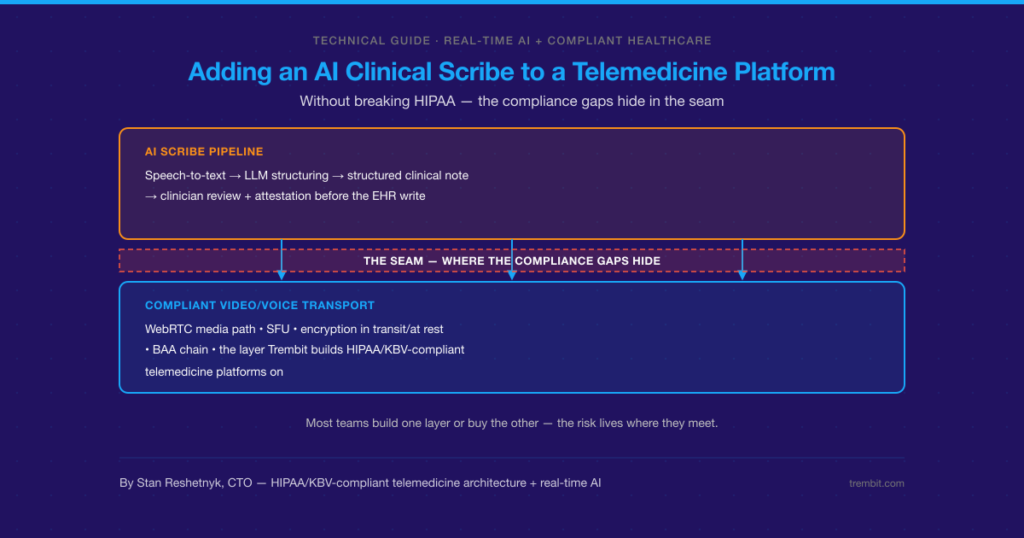
Building VR-Enabled Telehealth: The Technology Layer
Organizations pursuing any of the validated use cases above face a common challenge: integrating VR platforms with existing telehealth infrastructure in a way that is compliant, maintainable, and clinically usable.
This is where the engineering complexity lives. Connecting a VR session platform to a patient record, enabling a clinician to monitor and adjust a session in real time, transmitting session metrics to a care team dashboard, ensuring data is encrypted and HIPAA-compliant end-to-end — none of this is trivial.
Trembit specializes in exactly this kind of complex, compliance-forward healthcare software integration. With deep experience in telehealth platform development, real-time video infrastructure, and clinical data systems, Trembit helps healthcare organizations move from a validated VR use case to a deployed, integrated product — without the engineering detours that come from working with teams unfamiliar with healthcare’s technical and regulatory constraints.
Whether you are evaluating a commercial VR platform for integration, building proprietary VR-enabled telehealth tooling, or assessing what the right technology investment looks like for your patient population, Trembit brings the expertise to make that process rigorous and efficient.
Conclusion
VR in telemedicine is past the hype phase and into the evidence phase. The honest picture is one of specific, well-defined areas of genuine clinical value — mental health treatment, pain management, rehabilitation, surgical planning, and training — alongside a wider landscape of applications that are not yet ready for routine clinical deployment.
The organizations that will benefit most from VR in telemedicine are those that start with a clinical problem, find the application where VR’s specific strengths match the therapeutic mechanism, and build or integrate the technology with the same rigor they would apply to any clinical tool.
The technology is ready, in the right places. The question is whether the clinical workflows, reimbursement models, and engineering infrastructure are ready alongside it.