Telemedicine MVPs frequently collapse after launch — not because the idea is weak, but because the underlying architecture can’t support real-world healthcare demands. Scalability gaps, poor interoperability, and compliance blind spots drive high churn, provider abandonment, and investor hesitation. Industry data shows that up to 80% of telehealth MVPs fail within the first year when these risks are ignored.
Trembit helps founders and CTOs turn fragile prototypes into production-grade platforms by designing scalable, compliant, and integration-ready architectures from day one — often doubling post-launch survival rates.
The Most Common Reasons Telemedicine MVPs Fail
While the symptoms of failure vary from product to product, the underlying causes are surprisingly consistent. Understanding these patterns early helps founders avoid repeating the same architectural mistakes that derail most telemedicine MVPs.
1. Flashy Features, Fragile Foundations
Many MVPs prioritize visible features — video calls, AI symptom checkers, or dashboards — while underinvesting in backend resilience. The result is predictable:
- Video sessions degrade or crash during peak hours.
- Scheduling systems desync
- Trust erodes after the first bad clinical experience.
Once clinicians lose confidence, adoption rarely recovers.
2. No EHR/EMR Integration = Provider Drop-Off
Telemedicine platforms that don’t integrate with EHR/EMR systems require clinicians to perform double documentation. This leads to:
- 40–60% provider churn within months
- Workflow fragmentation
- Rejection by enterprise healthcare networks
Without interoperability (FHIR-based APIs, HL7 mappings), even well-designed apps face resistance from care teams.
3. Betting Everything on Pandemic-Only Demand
MVPs built exclusively for pandemic-era demand failed to adapt when in-person care rebounded. Platforms without:
- Hybrid care flows
- Remote monitoring extensions
- Chronic or behavioral health continuity
Quickly stagnated, as seen with several high-profile telehealth providers post-2021.
4. Feature Creep That Burns Runway
Overbuilding is one of the fastest ways to kill an MVP. Each unnecessary feature can add $ 30,000–$ 70,000 in development costs, delaying launch and exhausting budgets before product-market fit is validated.
Instead of learning from real users, teams ship bloated products with unclear value propositions.
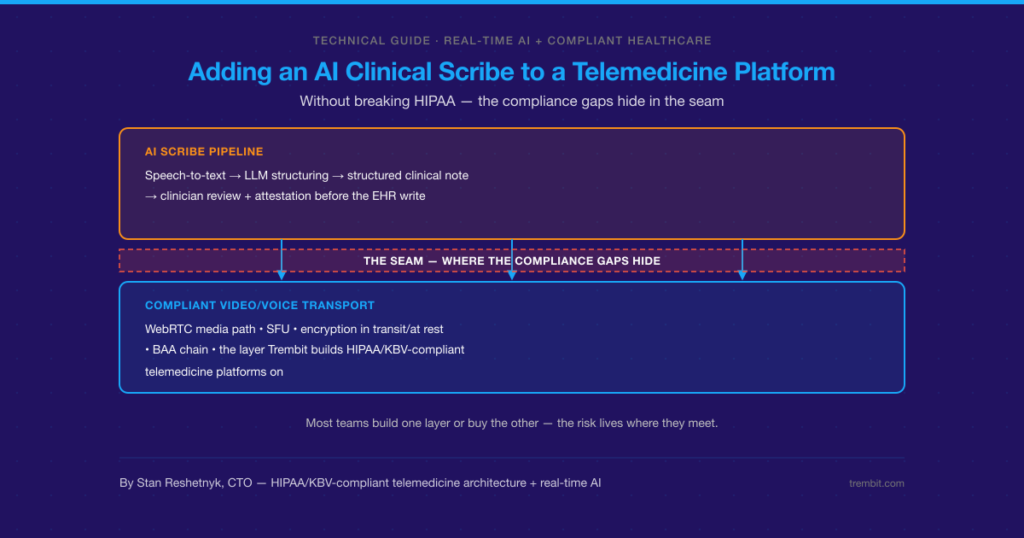
5. Compliance as an Afterthought
Security and regulatory gaps are fatal in healthcare. MVPs that delay HIPAA, FHIR, or data governance considerations face:
- Failed audits
- Blocked partnerships
- Immediate enterprise disqualification
Over 70% of unsuccessful telemedicine launches cite trust, privacy, or compliance issues as a primary factor.
Why Architecture Determines Survival
Once the initial failure triggers are clear, the next question becomes obvious: what actually separates telemedicine MVPs that survive from those that quietly disappear? In nearly every successful case, the answer is architecture.
Modular, Scalable System Design
Successful telemedicine platforms are built on:
- WebRTC for low-latency, high-reliability video
- Microservices for scheduling, video, billing, and notifications
- Independent scaling of high-load components
This approach reduces latency by up to 50% and enables 10× user growth without re-architecture.
Interoperability by Default
Architecture that integrates with systems like Epic, Cerner, or custom EHRs via standardized APIs increases clinician adoption and long-term retention. Providers are far more likely to embrace platforms that fit seamlessly into existing workflows.
Lean MVP Core Instead of Technical Debt
High-survival MVPs focus on three pillars only:
- Activation (first successful consultation)
- Retention (repeat usage by patients and providers)
- Compliance (security and audit readiness)
By resisting premature complexity, teams avoid the technical debt that cripples 60% of healthtech products later.
Event-Driven, Real-Time Architectures
Trembit helps clients implement event-driven systems that support:
- Real-time vitals monitoring
- AI-assisted triage
- Alerting and escalation workflows
This foundation enables safe scaling into chronic care and behavioral health use cases—key drivers of long-term platform viability.
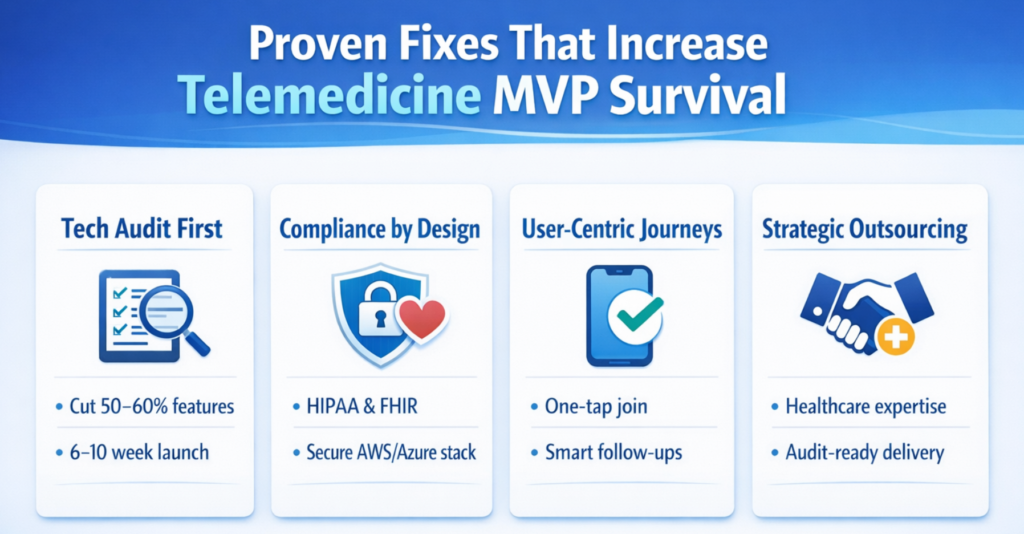
Proven Fixes That Increase MVP Survival
The good news is that these failures are not inevitable. Teams that address architectural risks early—before scaling or fundraising—dramatically increase their odds of long-term success. Below are proven, repeatable fixes Trembit applies when stabilizing or rebuilding telemedicine MVPs.
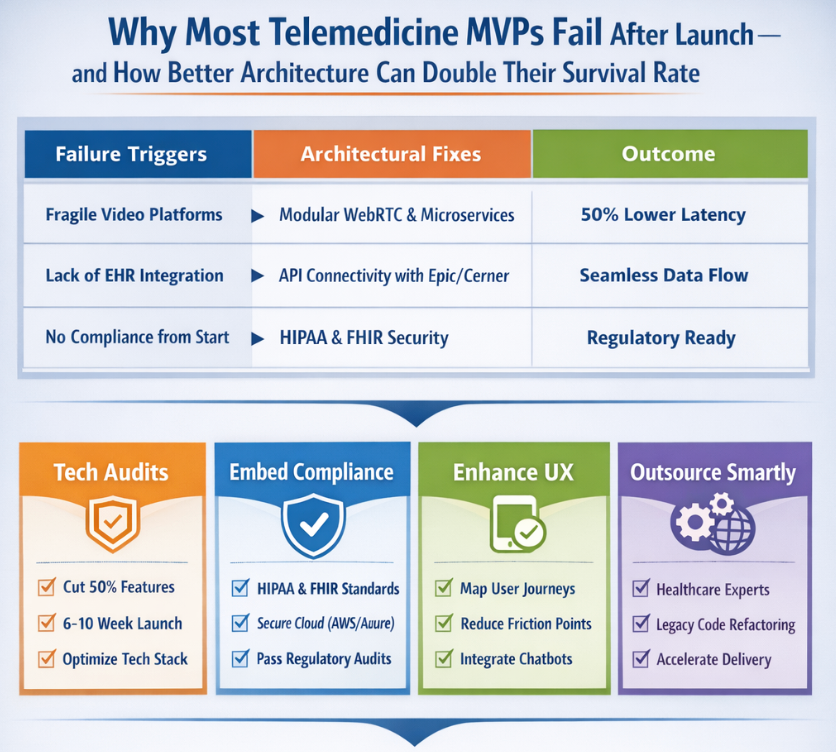
Quick Reference: Failure Triggers vs. Architectural Fixes
| Failure Trigger | Business Impact | Architectural Fix | Outcome |
| Backend instability under load | Session drops, lost trust | WebRTC tuning + autoscaling microservices | Stable video at peak traffic |
| No EHR/EMR integration | 40–60% provider churn | FHIR-based APIs, HL7 mappings | Higher clinician adoption |
| Feature creep | $30K–$70K wasted per feature | Lean MVP scope, modular services | Faster launch, lower burn |
| Compliance gaps | Failed audits, blocked deals | HIPAA-first cloud architecture | Enterprise readiness |
| Monolithic architecture | Costly rework, slow scaling | Event-driven microservices | 10× scalable growth |
Conduct a Technical Audit Before Scaling
A structured product–technology audit can eliminate 50–60% of non-essential features, enabling launches in 6–10 weeks instead of months.
Audit checklist includes:
- Load and stress testing of video and scheduling
- Architecture review (monolith vs. modular)
- Security and data flow mapping
- Integration readiness (EHR, billing, devices)
- Cloud cost and scaling assumptions
A structured product–technology audit can eliminate 50–60% of non-essential features, enabling launches in 6–10 weeks instead of months.
Build Compliance Into the Stack From Day One
HIPAA- and FHIR-aligned architectures using AWS or Azure prevent regulatory dead ends and accelerate enterprise onboarding.
Key compliance components to include:
- Encrypted data at rest and in transit
- Role-based access control (RBAC)
- Audit logs and traceability
- Secure identity and session management
- Business Associate Agreement (BAA)-ready infrastructure
HIPAA- and FHIR-aligned architectures using AWS or Azure prevent regulatory dead ends and accelerate enterprise onboarding.
Design Around Real User Journeys
Mapping patient and clinician journeys reveals friction in:
- Mobile UX
- Scheduling flows
- Post-consult follow-ups
High-impact journey optimizations:
- One-tap appointment join for patients.
- Auto-filled clinical notes via EHR sync
- Smart reminders and follow-up tasks
- Context-aware chat (pre- and post-visit)
Automation (e.g., chatbots) should support, but not replace, human empathy.
Mapping patient and clinician journeys reveals friction in:
- Mobile UX
- Scheduling flows
- Post-consult follow-ups
Outsource Strategically, Not Cheaply
Healthcare-focused teams like Trembit bring:
- Domain expertise
- Audit-ready development practices
- Legacy code refactoring experience
What to expect from a specialized partner:
- Faster MVP-to-production transition
- Lower long-term maintenance costs
- Reduced audit and compliance risk
- Architecture designed for future AI and RPM extensions
Healthcare-focused teams like Trembit bring:
- Domain expertise
- Audit-ready development practices
- Legacy code refactoring experience
This results in faster launches, smoother compliance reviews, and lower long-term costs.
Why Founders Choose Trembit
After working with dozens of telemedicine teams, a clear pattern emerges: founders don’t fail because they lack vision — they fail because their technology can’t keep up with clinical, regulatory, and operational realities. This is where Trembit consistently delivers value. Trembit specializes in rescuing and scaling complex telemedicine MVPs through:
- Architecture audits
- WebRTC-optimized video systems
- Modular, compliance-first builds
Clients across chronic care and behavioral health avoid common pitfalls and achieve 2× higher post-launch survival rates by relying on Trembit’s battle-tested approach.
Ready to Strengthen Your Telemedicine MVP?
Architecture problems rarely announce themselves early. They surface later — during audits, traffic spikes, or enterprise negotiations — when fixes are most expensive. Addressing them now is the difference between a short-lived MVP and a platform built to last. If your MVP struggles with scalability, compliance, or adoption — or if you want to avoid these risks entirely — Trembit can audit your architecture and prepare your platform for long-term growth.