Most telehealth founders carefully plan for the obvious expenses — development time, software licensing, and marketing costs. Then the AWS bill arrives three months after launch and resets every assumption. Infrastructure costs in healthcare software have a way of compounding silently, driven by compliance requirements, data retention obligations, and the particular demands of real-time medical communication.
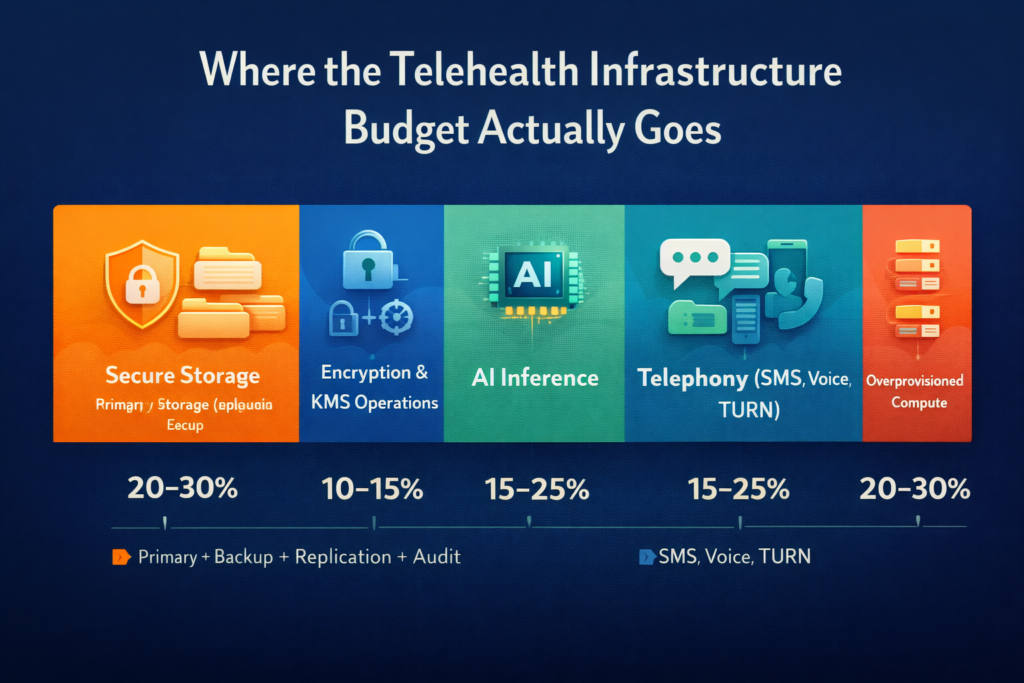
The problem isn’t that telehealth infrastructure is inherently expensive. It’s what hides in places non-specialists don’t anticipate. Encrypted storage is billed at multiple layers. AI inference charges that scale with clinical volume. Telephony costs that dwarf video infrastructure. And the most insidious culprit — overprovisioned infrastructure justified by compliance anxiety rather than actual requirements.
This article breaks down where money actually goes in telehealth infrastructure, and how cost-aware architecture can dramatically reduce spend without compromising security or compliance.
Secure Storage: Paying Multiple Times for the Same Data
At first glance, healthcare data storage seems straightforward — store patient records and access them when needed. In reality, HIPAA compliance turns storage into a multi-layered cost structure that many founders only fully understand once they start receiving infrastructure bills.
The Compliance Storage Stack
A single patient intake form is not stored in just one place. In a properly designed HIPAA-compliant system, it may be stored across multiple layers at the same time — primary encrypted storage, daily automated backups, cross-region disaster recovery copies, and audit log storage. Each of these layers adds its own cost, and each is required to meet compliance standards.
The multiplication effect is significant. If your primary storage costs $0.023 per GB (standard S3 pricing), your total effective storage cost might reach $0.08 to $0.12 per GB when backup, replication, and audit storage are factored in. For platforms with significant document storage — intake forms, lab results, clinical notes, session recordings — this compounds quickly.
Reducing Storage Costs Without Reducing Compliance
One of the most overlooked cost controls is data lifecycle management. Not all data needs to stay in the same storage tier for its entire retention period.
For example, an intake form that is actively used during a patient’s treatment should remain in fast (and more expensive) storage. But that same form, three years later — kept only to satisfy regulatory requirements — can be moved to low-cost archive storage.
Cloud providers make this easy to automate.
- AWS S3 Intelligent-Tiering
- Azure Blob lifecycle policies
- Google Cloud Storage lifecycle management
These tools automatically move data based on access patterns. For instance, data not accessed for 90 days can shift to infrequent access storage. After 180 days, it can move to archive storage. The data remains secure and compliant — it just takes seconds instead of milliseconds to retrieve, which is perfectly acceptable for historical records.
Another underused cost-saving strategy is compressing documents before encryption. Clinical records — especially text-heavy documents and structured form data — compress very well. Compression must happen before encryption (because encrypted data cannot be compressed effectively). This step alone can reduce storage size by 40–60% for text-heavy content.
Encrypted File Handling: The Processing Tax
Encryption is non-negotiable in healthcare. But encryption operations aren’t free — they consume compute resources during every upload, download, and processing operation. In high-volume platforms, this processing tax becomes material.
Where Encryption Costs Accumulate
Client-side encryption, server-side encryption, and encryption in transit each add processing overhead. The costs are individually small but accumulate at scale. A platform processing 10,000 document uploads daily, each requiring key retrieval from an HSM, encryption operation, and secure storage, faces different economics than a platform at 100 uploads daily.
Key management services add their own cost layer. AWS KMS charges per API call for cryptographic operations. At a meaningful scale — millions of monthly operations — these charges become a significant budget line.
Practical Optimization Strategies
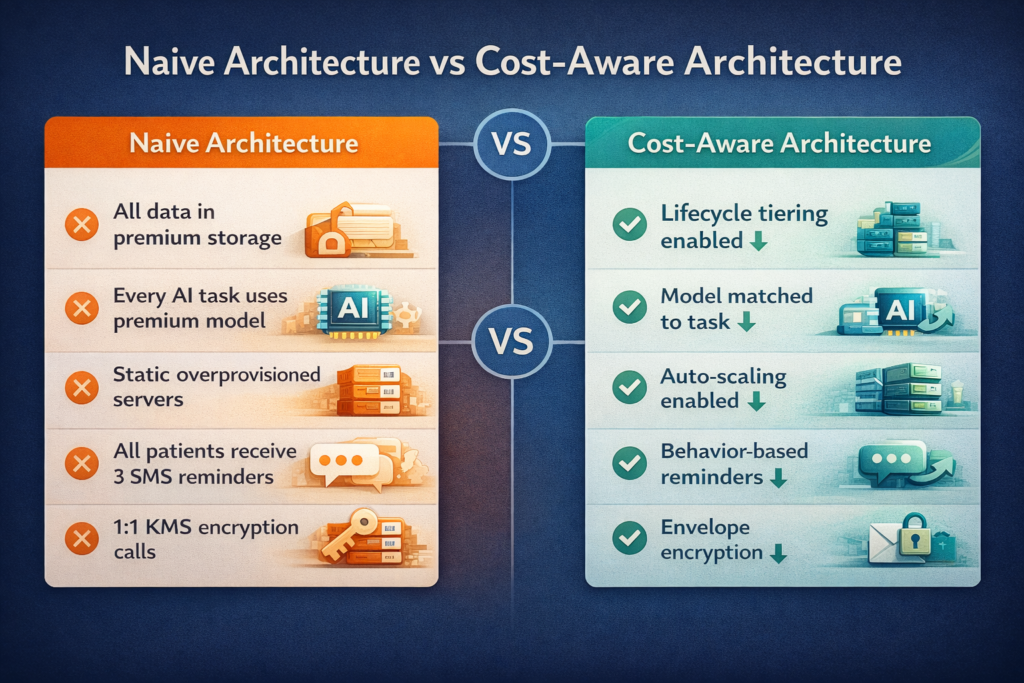
Envelope encryption reduces KMS API calls dramatically. Rather than encrypting every data element individually with your KMS-managed key, encrypt data with locally generated data keys, then encrypt only those data keys with KMS. The ratio of KMS calls to encryption operations shifts from 1:1 to something closer to 1:1000, cutting KMS costs proportionally.
Batching small file operations reduces per-operation overhead. Rather than processing uploaded files individually, queue them for batch processing during low-traffic periods. The same encryption work happens — it’s just scheduled efficiently rather than on-demand.
AI Inference Costs: The Budget Item Nobody Planned For
AI inference costs are the fastest-growing infrastructure line item for telehealth platforms in 2026. Clinical documentation AI, triage assistants, and predictive analytics all consume inference budget at rates that surprise founders who scoped costs using basic API pricing.
Why AI Costs Exceed Projections
API pricing for AI models is quoted per token — a unit that loosely maps to words. Clinical text is token-dense. A single patient visit note might contain 1,500 tokens of input context plus 800 tokens of output. At $0.003 per 1,000 tokens (mid-tier model pricing), that’s less than a cent per note. Across 500 daily patient visits, that’s around $1.50 daily — seemingly negligible.
The problem is multiplier effects. Clinical documentation AI doesn’t process a visit once. It processes drafts, revisions, and structured extraction separately. If a physician iterates on an AI-generated note three times, token consumption triples. If your platform generates AI summaries for care coordinators in addition to clinical notes, consumption doubles again. Real-world inference costs often run five to ten times naive projections.
Cost-Aware AI Architecture
The single most effective cost control is model selection by task. Not every AI task requires the most capable — and most expensive — model. Clinical documentation that requires nuanced medical reasoning justifies premium model pricing. Classifying appointment types or extracting structured data from forms works fine with smaller, cheaper models at one-tenth the cost.
| AI Task | Recommended Tier | Relative Cost | Justification |
| Clinical note generation | Premium (GPT-4, Claude Sonnet) | High | Medical accuracy critical |
| Symptom triage classification | Mid-tier | Medium | Structured output, lower stakes |
| Appointment type extraction | Small / fine-tuned | Low | Simple classification task |
| Patient FAQ responses | Mid-tier | Medium | Quality matters, not critical |
| Document summarization | Mid-tier | Medium | Balance quality and cost |
| Form field extraction | Small / rules-based | Lowest | Structured data, no reasoning needed |
Caching AI responses eliminates redundant inference entirely. Many AI tasks in telehealth are effectively deterministic — the same clinical context produces the same useful output. If your platform generates pre-visit summaries, and a provider views the same patient’s summary three times, you should be paying for one inference operation, not three. Response caching with appropriate invalidation logic can reduce inference costs by 30 to 50 percent on high-traffic platforms.
Prompt optimization reduces token consumption without reducing output quality. Verbose system prompts padded with redundant instructions are a common cost source. Auditing token consumption by prompt component — and ruthlessly trimming redundant context — often reduces input tokens by 20 to 30 percent with no quality impact.
Telephony Expenses: The Underestimated Line Item
Video consultation infrastructure is the visible telephony cost in telehealth. But the full telephony picture includes SMS notifications, voice fallback for poor video connections, automated reminder calls, and PSTN integration for patients without smartphone access.
Telephony costs scale directly with clinical volume and don’t compress the way storage or compute costs do. Each SMS, each voice minute, each PSTN connection has a floor cost that discounting and optimization can reduce but not eliminate.
Video Infrastructure Choices
Building video infrastructure directly on WebRTC using cloud media servers (such as Twilio, Vonage, or Amazon Chime SDK) gives you more cost control than using packaged telehealth video solutions.
Per-minute pricing works well when session lengths are relatively predictable and average in duration. However, if session times vary widely — for example, some visits last two minutes while others last ninety — committing to minimum usage tiers can lead to unnecessary spending.
The decision between running your own TURN servers or relying on managed media infrastructure depends largely on your patients’ network conditions.
- Patients on stable broadband connections typically connect peer-to-peer using WebRTC, avoiding per-minute relay costs.
- Patients on mobile networks or behind restrictive NAT configurations often require TURN relay, which introduces additional bandwidth expenses.
Understanding your patient population’s network reliability before selecting your video infrastructure helps avoid choosing a cost model that doesn’t match your real-world usage.
SMS Optimization
Notification SMS costs seem trivial individually — fractions of a cent per message — but high-volume appointment reminders accumulate meaningfully. A platform sending three reminder messages per appointment across 1,000 daily appointments sends 90,000 monthly SMS messages. At $0.0075 per message, that’s $675 monthly just for appointment reminders.
Intelligent reminder logic reduces volume without reducing effectiveness. Rather than time-based reminders sent regardless of patient behavior, send reminders only to patients who haven’t confirmed. Analyze no-show patterns by patient segment and adjust reminder frequency accordingly. A patient who has never missed an appointment needs fewer reminders than one with a history of no-shows.
Infrastructure Overprovisioning: The Compliance Tax
Perhaps the highest hidden cost in telehealth infrastructure is the one created by anxiety rather than requirements. Healthcare compliance creates legitimate performance and reliability requirements — but it doesn’t require overprovisioned infrastructure running at 15 percent utilization.
The pattern is consistent: developers unfamiliar with healthcare compliance provision infrastructure defensively, justifying over-allocation with vague compliance reasoning. Production databases run on instances sized for 10x actual load. Application servers maintain minimum instance counts that handle peaks comfortably but waste budget during off-hours. Redundant services run in active-active configurations that provide no compliance benefit over active-passive.
Right-Sizing Without Risk
The solution isn’t reducing reliability — it’s measuring before provisioning. CloudWatch, Azure Monitor, and Google Cloud Monitoring provide detailed resource utilization metrics. Reviewing 90-day utilization data typically reveals significant provisioning opportunities. Database CPU averaging 8 percent suggests you’re paying for capacity you don’t need. Application servers idling at 12 percent memory utilization can be right-sized or consolidated.
Auto-scaling addresses variable load more cost-efficiently than static overprovisioning. A telehealth platform has predictable traffic patterns — peak hours during business hours, low traffic overnight, and weekends. Auto-scaling groups that expand during business hours and contract overnight can reduce compute costs by 40 to 60 percent compared to static provisioning sized for peak load.
HIPAA compliance requires availability, not specific instance sizes. A right-sized infrastructure with proper redundancy — multi-AZ database deployment, load-balanced application tier, automated failover — meets compliance requirements at materially lower cost than oversized single-configuration deployments.
Building Cost Awareness Into Architecture
The most effective cost control happens at design time, not after invoices arrive. Cost-aware architecture means treating infrastructure spend as a first-class concern alongside security, performance, and compliance — making tradeoffs explicitly rather than discovering them in production.
Practical cost-aware architecture principles include establishing cost budgets per service component before implementation, reviewing infrastructure choices against cost implications during design reviews, instrumenting production systems with per-feature cost attribution so product decisions reflect true economics, and scheduling quarterly infrastructure audits to identify drift from optimized configurations.
At Trembit, cost-aware architecture is a core part of how we approach telehealth platform design. We’ve helped platforms reduce infrastructure costs by 35 to 55 percent through systematic audits — not by cutting compliance corners, but by replacing defensive overprovisioning with properly measured, right-sized infrastructure. We understand that compliance requirements and cost efficiency aren’t opposing forces. Thoughtful architecture serves both.
The Compounding Returns of Getting This Right
Infrastructure cost optimization in telehealth isn’t a one-time project — it’s an ongoing discipline with compounding returns. Platforms that establish cost-aware architecture early make better product decisions, price their services more competitively, achieve profitability at lower revenue thresholds, and have more capital available for product development.
The founders who treat infrastructure costs as a strategic concern — not just an operational one — build more durable businesses. They understand where every dollar of cloud spend goes, what compliance actually requires versus what anxiety has imposed, and how to scale efficiently rather than expensively.
The hidden costs of telehealth infrastructure become visible once you know where to look. And visible costs are controllable ones.