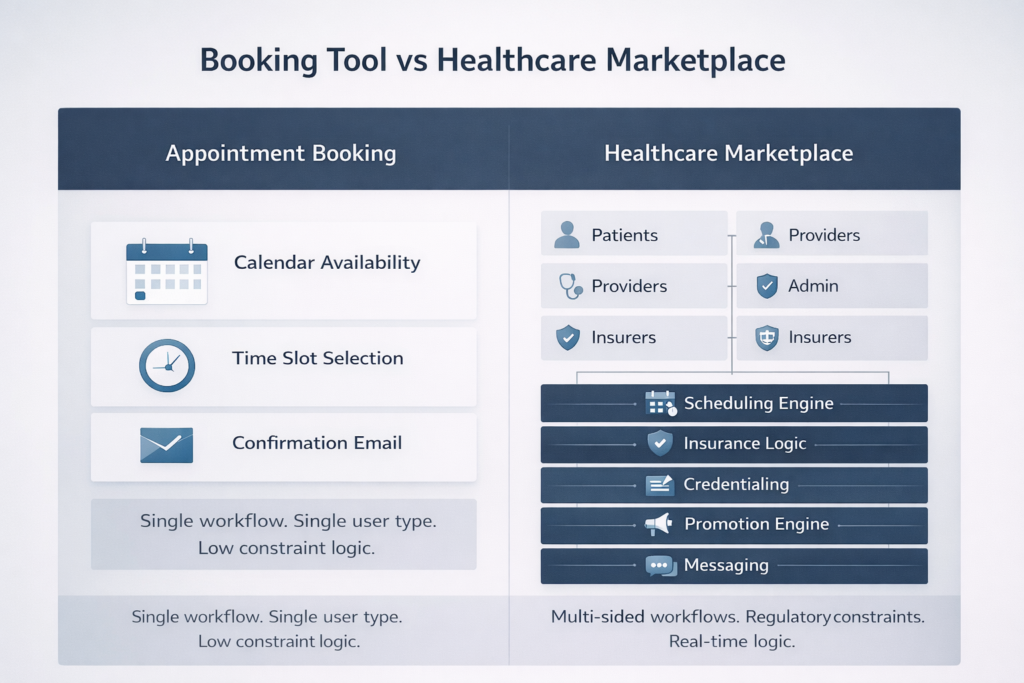
A simple appointment booking system is a solved problem. Calendar availability, time slot selection, confirmation email — dozens of off-the-shelf tools handle this adequately. A healthcare marketplace that connects patients with providers across specialties, insurance networks, and care modalities while managing promotions, verifying credentials, and enforcing clinical workflows is an entirely different engineering challenge.
The distinction matters because founders frequently underestimate the architectural distance between these two things. They start with booking, add features incrementally, and eventually find themselves maintaining a fragile system that barely holds together under the weight of requirements it wasn’t designed to support. The path from appointment booking to healthcare marketplace requires deliberate architectural thinking from the beginning — not a feature roadmap, but a platform architecture.
Understanding the Multi-Sided Nature of Healthcare Marketplaces
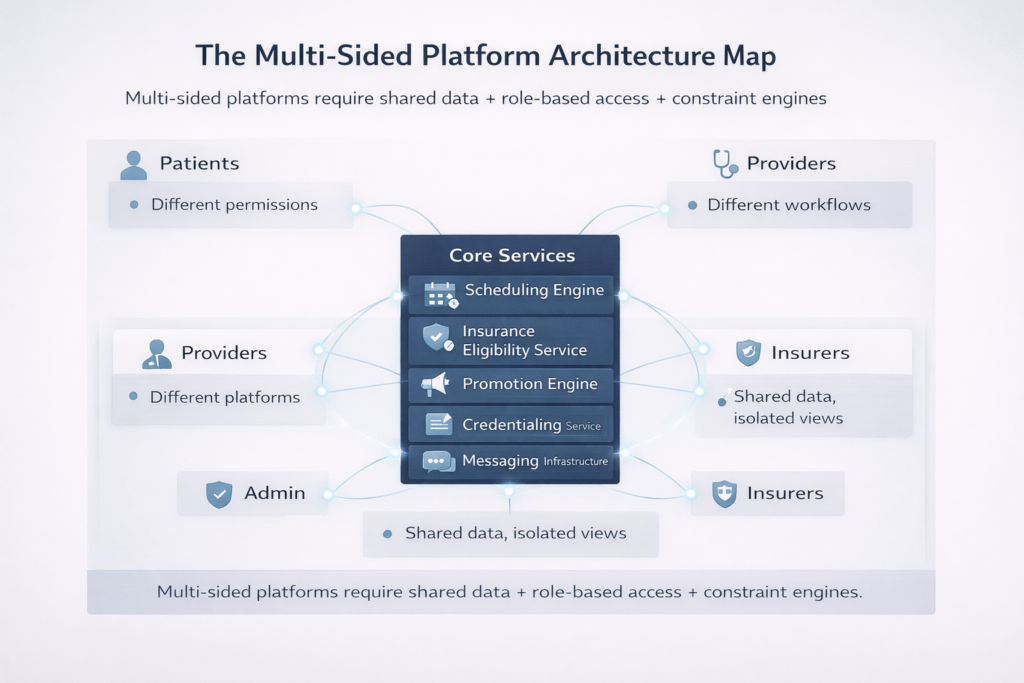
Marketplaces succeed when they create value for every participant simultaneously. Healthcare marketplaces serve at least three distinct constituencies — patients, providers, and administrators — each with fundamentally different needs, different data access requirements, and different workflows. A fourth side, insurers and payers, adds further complexity in platforms that handle insurance verification and claims.
Each side of the marketplace has its own mental model of what the platform is. To a patient, it’s a way to find and access care. To a provider, it’s a practice management tool and patient acquisition channel. To an administrator, it’s an operational control center. To an insurer, it’s a claims and eligibility interface. Your architecture must serve all of these simultaneously without privileging any one at the expense of others.
The technical challenge is that these constituencies share data — appointments, clinical records, billing information — but require different views, different access controls, and different interaction patterns for the same underlying data. A patient and a provider both interact with the same appointment entity, but they see different fields, trigger different workflows, and have different permissions to modify it.
Patient Dashboard: Designing for Trust and Simplicity
The patient dashboard is the marketplace’s front door. Its primary job is to reduce the friction between a patient recognizing a healthcare need and successfully accessing care. Secondary jobs include maintaining continuity across episodes of care, facilitating communication with providers, and managing the administrative complexity of insurance and billing.
The core patient dashboard architecture centers on a unified timeline — a chronological view of past, present, and upcoming interactions with the platform. Upcoming appointments, outstanding intake forms, pending lab results, prescription renewals, and unread messages from providers all surface in this timeline with appropriate urgency signals.
Key patient dashboard capabilities that distinguish healthcare-grade platforms from generic booking tools include the following:
- Provider matching based on specialty, insurance acceptance, language preference, location, and availability — not just calendar lookup
- Intake form management with save-and-resume functionality and a clear indication of what’s required before each appointment
- Insurance card storage with eligibility verification status displayed transparently.
- Appointment preparation content delivered in the days before a visit, customized to appointment type and provider preference
- Post-visit continuity, including follow-up task tracking, prescription status, and care plan adherence support
- Secure messaging with read receipts, file attachment support, and clear routing to the appropriate care team member
The patient dashboard must be designed with health literacy in mind. Patients navigating a healthcare marketplace during moments of stress or illness need interfaces that are unambiguous, forgiving of errors, and accessible across devices and connection qualities. This is a design constraint with architectural implications — it pushes toward progressive disclosure of complexity, robust offline support, and graceful degradation on poor network connections.
Provider Dashboard: Balancing Clinical and Operational Needs
Providers interact with the platform in fundamentally different contexts than patients. A physician, between consultations, has seconds to review an incoming patient’s intake summary. An administrative coordinator has minutes to verify insurance eligibility before a scheduled appointment. A practice manager has an ongoing need to analyze scheduling efficiency and revenue trends.
The provider dashboard must serve all of these contexts, which means it cannot be a single interface. It needs distinct modes or views optimized for different task types — a clinical mode focused on patient information and consultation tools, an operational mode focused on scheduling and workflow management, and an analytics mode focused on practice performance.
Core provider dashboard requirements that go beyond basic scheduling tools:
- Pre-visit preparation view surfacing patient’s history, intake responses, outstanding items, and clinical context before a consultation begins
- Real-time schedule management with drag-and-drop rescheduling, buffer time controls, and instant availability updates reflected across all patient-facing booking surfaces
- Earnings and payout tracking with a transparent breakdown of platform fees, insurance reimbursements, and direct pay amounts
- Credential and license management with expiration alerts and streamlined renewal documentation upload
- Patient communication tools integrated with the messaging system, with template support for common post-visit communications
- Referral management enables providers to refer patients to colleagues within the platform and track referral outcomes.
Provider dashboard performance requirements are more demanding than patient dashboard requirements. Providers in active consultation workflows cannot tolerate slow page loads or unreliable real-time updates. The architecture must prioritize low-latency data delivery for provider-facing interfaces, using WebSocket connections for real-time schedule updates and optimistic UI patterns for actions that modify appointment state.
Admin Dashboard: Operational Intelligence at Scale
The administrative layer of a healthcare marketplace is where operational complexity concentrates. Clinic administrators, platform operators, and compliance officers each need control surfaces that give them visibility and intervention capability without creating security risks.
The admin dashboard architecture requires role-based access that’s more granular than most platforms implement. A clinic administrator should be able to manage their clinic’s providers and schedules without seeing other clinics’ data. A compliance officer needs audit trail access without operational control capabilities. A platform operator needs system-wide visibility without the ability to modify clinical records.
Key admin dashboard capabilities that enterprise customers evaluate during procurement:
| Capability | Clinic Admin | Platform Operator | Compliance Officer |
| Provider credential management | Own clinic only | All clinics | Read-only |
| Schedule configuration | Own clinic only | All clinics | No access |
| Patient record access | Own clinic only | Emergency only | Audit logs only |
| Insurance contract management | Own clinic only | All clinics | Read-only |
| Audit log review | Own clinic only | All systems | All systems |
| Platform configuration | No access | Full access | No access |
| Financial reporting | Own clinic only | Aggregated view | No access |
The admin dashboard is also where platform health monitoring surfaces. Appointment completion rates, provider utilization, intake form abandonment, insurance verification failure rates, and payment processing errors all need operational visibility. Dashboards that surface these metrics in real time enable administrators to intervene before problems compound — a provider with an unusually high no-show rate needs a different response than a sudden spike in insurance verification failures.
Promotion Engine: Healthcare-Grade Incentive Architecture
Promotions in healthcare marketplaces are more constrained than in consumer e-commerce, but they’re not absent. First-visit discounts for new patients, reduced-rate consultations for underserved populations, promotional pricing for newly onboarded providers building their patient panels, and employer-sponsored visit benefits all require promotion engine infrastructure.
The promotion engine architecture must handle several healthcare-specific constraints that generic coupon systems don’t accommodate. Promotions cannot apply to services covered by insurance — applying a discount to an insurance-covered visit creates billing compliance issues. Promotions must be compatible with provider compensation agreements. Certain promotion types are prohibited under anti-kickback statutes for specific service categories.
The technical architecture typically involves a promotion eligibility service that evaluates promotion applicability at booking time, considering patient insurance status, service type, provider participation agreements, and applicable regulatory constraints before presenting promotion options.
Core promotion engine capabilities include:
- Eligibility rules engine supporting complex conditions: new patient only, specific specialty, specific insurance status, employer group membership, geographic region
- Stacking rules defining which promotions can combine and which are mutually exclusive
- Provider participation controls, allowing providers to opt into or out of specific promotions affecting their services
- Redemption tracking with clear audit trails for compliance and financial reconciliation
- Expiration and capacity management for time-limited or volume-limited promotional campaigns
Insurance Logic: The Complexity That Defines Healthcare Marketplaces
Insurance integration is what most clearly separates a healthcare marketplace from a generic booking platform. It’s also the area where architectural shortcuts create the most persistent technical debt.
The insurance logic layer must handle real-time eligibility verification, benefit determination, cost-sharing calculation, and claims submission — each of which involves integrations with payers, clearinghouses, and provider credentialing databases that are inconsistent, occasionally unavailable, and frequently updated without notice.
Real-time eligibility verification uses X12 270/271 transactions (or REST equivalents through clearinghouse APIs like Change Healthcare or Availity) to verify a patient’s active coverage and retrieve benefit details before an appointment. The result must be cached intelligently — verification valid for the current day, invalidated if the patient’s insurance information changes, with fallback behavior when verification fails.
Cost-sharing calculation translates raw benefit information into patient-facing cost estimates. This requires understanding deductible accumulation (how much of the deductible has been met in the current benefit year), out-of-pocket maximum tracking, copay versus coinsurance structures, and service-specific benefit exceptions. Getting this calculation wrong — even in the patient’s favor — creates trust and reconciliation problems.
The insurance logic layer requires a dedicated architectural component rather than distributed insurance handling across booking, billing, and patient-facing code. Centralizing insurance logic in a dedicated service ensures consistency, simplifies compliance with payer contract terms, and isolates the complexity of insurance rules from the rest of the platform.
Scheduling Logic: Beyond Calendar Availability
Scheduling in a healthcare marketplace involves constraints that general-purpose calendar systems aren’t designed to handle. Provider availability is not simply a matter of open time slots — it involves license jurisdiction (a provider can only see patients in states where they’re licensed), appointment type constraints (not every provider performs every service type), care continuity rules (returning patients may require the same provider), and regulatory requirements (certain telehealth services require prior in-person visits in specific states).
The scheduling engine architecture requires a constraint satisfaction approach — given a patient’s requirements and preferences, find available providers satisfying all applicable constraints and rank them by match quality.
Core scheduling constraints that healthcare-grade platforms must enforce include:
- Jurisdiction matching verifies that the provider holds an active license in the patient’s state at the time of the appointment.
- Credential-to-service matching ensures that the appointment type is within the provider’s scope of practice and platform credentialing.
- Insurance network matching filtering providers to those participating in the patient’s insurance network when relevant
- Appointment type duration rules apply service-specific duration defaults that override generic slot lengths.
- Buffer time enforcement, respecting provider-configured preparation and documentation time between appointments
- Care continuity preferences preferentially route returning patients to their established provider when available.
The scheduling engine must handle these constraints in real time during the booking flow, returning available options within acceptable latency while evaluating potentially dozens of constraints per provider. This requires intelligent caching of constraint-stable data (license status, insurance network participation) while computing constraint-volatile data (current availability) dynamically.
Bringing the Architecture Together
Multi-sided telehealth marketplaces succeed when the architectural decisions serving each side of the platform reinforce rather than compromise each other. Patient-facing simplicity is achieved through backend complexity, not despite it. Provider operational efficiency depends on insurance logic accuracy. Admin oversight requires an audit infrastructure built into every other layer.
At Trembit, we’ve architected multi-sided telehealth platforms from the ground up — designing patient matching systems, building insurance eligibility pipelines, implementing promotion engines compliant with healthcare regulations, and creating scheduling constraint engines that handle real-world clinical complexity. We understand that the distance between a booking system and a healthcare marketplace is measured in architectural decisions, not feature additions.
The platforms that reach marketplace scale in telehealth share a common characteristic: their founders made the right architectural commitments early, before the complexity of the problem was fully visible. They built extensible scheduling engines instead of calendar wrappers. They designed insurance logic as a dedicated service instead of scattered billing code. They implemented multi-sided dashboards instead of a single shared interface.
Building a healthcare marketplace is one of the most architecturally demanding software challenges in the healthcare technology space. Done well, it creates a platform that generates compounding value for every participant — connecting patients with the right care, enabling providers to build sustainable practices, and giving operators the visibility to scale with confidence.