Most telehealth platforms begin with a focused product vision, typically centered on video consultations, patient scheduling, and clinical documentation. Then reality hits. The hospital network wants FHIR-based EHR integration. The enterprise clinic operates a Practice Management System that does not allow for negotiation of its data model. The sales team needs patient interactions to flow into the CRM. The AI layer needs real-time clinical context to function. Suddenly, your clean product architecture becomes a tangle of point-to-point integrations, inconsistent data models, and brittle webhooks held together by institutional knowledge.
This is integration chaos — and it’s the defining technical challenge of telehealth platforms in 2026. The organizations winning in this market aren’t the ones with the best individual features. They’re the ones that have figured out how to build coherent ecosystems from incompatible systems. That requires architectural thinking, not just integration of plumbing.
The Interoperability Problem Is Structural, Not Technical
Before diving into solutions, it’s worth understanding why integration remains hard despite decades of standardization efforts. Healthcare data exists in a fractured landscape of legacy systems, proprietary APIs, and competing standards. A single patient encounter might touch an EHR, a billing system, a scheduling platform, a patient portal, and a lab integration — each with different data models, authentication mechanisms, and update frequencies.
The structural challenge is coordination. It’s not that individual integrations are impossible — they’re not. The challenge is making dozens of integrations work together coherently, handling failures gracefully, and keeping data consistent across systems that don’t share a single source of truth.
FHIR (Fast Healthcare Interoperability Resources) represents the most serious attempt to solve this at the data model level. But FHIR adoption varies wildly, implementation quality is inconsistent, and FHIR alone doesn’t solve the coordination problem.
FHIR Integration Patterns: Beyond the Basics
FHIR R4 has become the de facto standard for modern healthcare integration, mandated by the CMS Interoperability Rule for payers and increasingly expected by enterprise health systems. But “supporting FHIR” can mean very different things depending on implementation depth.
RESTful FHIR vs. FHIR Subscriptions
Most implementations start with RESTful FHIR — request-response APIs for reading and writing clinical resources. Your platform queries a Patient resource, creates an Encounter, and updates an Observation. This covers the majority of integration use cases and is well-supported by major EHR vendors.
FHIR Subscriptions enable event-driven patterns. Rather than polling for updates, your platform registers interest in specific resource types and receives notifications when they change. A subscription to Appointment resources notifies your platform immediately when an appointment is created or modified in the EHR, enabling real-time synchronization without constant polling.
The practical challenge is EHR support. FHIR Subscriptions are part of the R4B and R5 specifications, and not all EHR vendors have implemented them robustly. Many enterprise integrations still rely on polling with intelligent backoff strategies — not ideal, but pragmatic.
Bulk FHIR for Analytics
For analytics, reporting, and AI model training, Bulk FHIR (FHIR R4 $export operation) provides efficient population-level data access. Rather than fetching individual resources, Bulk FHIR exports all resources of specified types for a defined patient population to file storage, then notifies your platform when export is complete.
This changes the economics of analytics integration. You’re no longer making thousands of individual API calls to build a patient cohort — you’re processing structured files containing complete clinical histories. Combined with your event streaming infrastructure, Bulk FHIR enables both real-time updates and periodic comprehensive synchronization.
SMART on FHIR for Authorization
SMART on FHIR standardizes OAuth 2.0 authorization for FHIR APIs, enabling your platform to request specific clinical data scopes on behalf of authenticated users. Rather than broad access to all patient data, your platform requests only the resources it needs — patient/Observation.read for accessing lab results, patient/MedicationRequest.read for medication history.
This granular authorization model aligns with HIPAA’s minimum necessary standard and gives patients meaningful control over what data your platform can access.

PMS Integration Reality: Pragmatism Over Purity
Practice Management Systems handle the operational backbone of clinical practices — scheduling, billing, eligibility verification, and claims processing. They’re also some of the least standardized systems in healthcare IT.
Unlike EHRs that increasingly expose FHIR APIs, many PMS platforms still rely on HL7 v2 messaging, proprietary REST APIs, or even file-based integration. Your architecture must accommodate this reality without creating fragile point-to-point integrations.
| PMS Integration Type | Protocol | Reliability | Real-Time? | Typical Use Cases |
| HL7 v2 Messages | TCP/MLLP | High (mature) | Near real-time | Scheduling, ADT events, results |
| Proprietary REST API | HTTPS | Variable | Yes | Custom per vendor |
| FHIR R4 API | HTTPS | Growing | Yes | Modern PMS platforms |
| File-Based (CSV/XML) | SFTP | Low | No (batch) | Legacy systems, billing exports |
| Database Direct | JDBC/ODBC | Fragile | Yes (polling) | Last resort, avoid in production |
The pragmatic approach is building an integration abstraction layer — an internal API that speaks your platform’s data model, backed by adapters for each PMS you need to support. When you add a new PMS integration, you build a new adapter, not a new integration across your entire codebase.
This adapter pattern becomes more valuable over time. PMS vendors change APIs, deprecate endpoints, and release breaking updates. Your adapters isolate these changes to specific components rather than propagating them across your platform.
CRM Downstream Sync: Closing the Patient Journey Loop
Healthcare CRM platforms — Salesforce Health Cloud, HubSpot with healthcare customizations, Microsoft Dynamics — have become critical infrastructure for patient acquisition, retention, and engagement. Telehealth platforms that sync clinical and operational data to CRM systems enable closed-loop patient journeys.
The integration pattern is fundamentally downstream — your telehealth platform is the system of record for clinical events, and CRM receives enriched, de-identified, or consent-gated updates.
Key synchronization events include appointment creation and completion, intake form submissions, patient satisfaction scores, care plan adherence metrics, and re-engagement triggers. Each event enriches the CRM’s patient profile, enabling care coordinators and marketing teams to act on clinical context without accessing PHI directly.
The compliance boundary is critical. CRM systems typically aren’t designed as HIPAA-covered systems, and many healthcare organizations don’t have BAAs with their CRM vendors. This means your sync logic must carefully filter what data crosses the boundary. Patient engagement metrics, appointment attendance rates, and anonymized care outcomes can flow to CRM. Clinical notes, diagnoses, and medication details stay within your HIPAA-compliant infrastructure.
Event Orchestration Layer: The Missing Architectural Piece
Individual integrations — FHIR, PMS, CRM, AI — are manageable in isolation. The architectural challenge is coordinating them reliably. An appointment booked in your platform needs to sync to the PMS, create a FHIR Encounter resource in the EHR, trigger an AI-powered pre-visit summary, and notify the care coordinator’s CRM record. All of these need to happen correctly, even when individual systems are temporarily unavailable.
This is what an event orchestration layer solves. Rather than direct synchronous calls between systems, your platform emits events — structured messages describing what happened — to a central message broker. Downstream systems subscribe to relevant events and process them independently.
The architecture typically involves an event streaming platform (Apache Kafka, AWS EventBridge, or Google Pub/Sub), a schema registry ensuring event structure consistency, dead letter queues capturing failed event processing for retry, and monitoring dashboards providing visibility into event flow across systems.
The key design principles for healthcare event orchestration are:
- Idempotency — processing the same event twice produces the same result, preventing duplicate records from retry logic.
- Event ordering — clinical events have temporal relationships that matter; your broker must preserve ordering within event streams.
- Schema versioning — as data models evolve, old events must remain processable; use backward-compatible schema evolution.
- Audit completeness — every event is logged immutably, creating a complete audit trail of system interactions.
- Failure visibility — failed event processing surfaces immediately in monitoring, not discovered hours later through data inconsistency.
API Security Best Practices: Securing the Ecosystem Perimeter
An interconnected ecosystem dramatically expands your attack surface. Each integration is a potential entry point. Each API credential is a potential compromise vector. Healthcare data flowing between systems creates exposure opportunities that don’t exist in isolated platforms.
Securing this ecosystem requires layered controls applied consistently across all integrations:
Authentication and authorization use OAuth 2.0 with short-lived access tokens for all API integrations. Service-to-service authentication uses client credentials flow with per-integration credentials — never shared API keys. Implement PKCE for any integrations involving user-facing authorization flows.
Network-level controls restrict integration traffic to known IP ranges using allowlists. Internal integrations between your own services use mutual TLS (mTLS), ensuring both parties authenticate each other. External integrations traverse dedicated VPC endpoints or private network links where possible.
Input validation treats all data received from external systems as untrusted. Every FHIR resource, PMS message, and CRM webhook undergoes schema validation before processing. Unexpected fields are rejected, not silently ignored — they could indicate API changes or injection attempts.
Rate limiting and circuit breakers protect your platform from misbehaving integrations. Rate limits prevent a runaway integration from exhausting your resources. Circuit breakers automatically pause integrations that are repeatedly failing, preventing cascade failures from propagating across your system.
Credential rotation automates the regular rotation of all integration credentials. No integration credential should be older than 90 days. Automated rotation with zero-downtime key exchanges ensures security without operational disruption.
Monitoring and anomaly detection establish baseline traffic patterns for each integration and alert on deviations. A FHIR integration that suddenly requests 10x normal data volume might indicate a misconfiguration — or a compromised credential being used for data exfiltration.
Bringing It Together: Ecosystem Over Features
The telehealth platforms that will define the next five years aren’t the ones with the most features — they’re the ones that function as coherent ecosystems. They’re the platforms where data flows correctly from patient intake through clinical care to billing and follow-up. Where AI systems have the real-time clinical context they need. Where enterprise customers can integrate with their existing infrastructure without multi-month implementation projects.
Building this requires architectural vision that most feature roadmaps don’t address. It requires thinking about data models, event flows, integration abstractions, and security boundaries — not just user stories and sprint velocity.
At Trembit, we specialize in exactly this kind of ecosystem architecture for telehealth platforms. We’ve designed and implemented FHIR integration layers supporting multiple EHR vendors, built PMS adapter frameworks that isolate proprietary protocol complexity, architected event orchestration systems handling millions of clinical events daily, and established API security frameworks meeting enterprise procurement requirements.
We understand that integration work isn’t glamorous — it doesn’t appear on marketing pages or demo videos. But it’s what separates telehealth platforms that enterprise customers trust with their infrastructure from those that remain departmental tools. It’s the difference between a product and a platform.
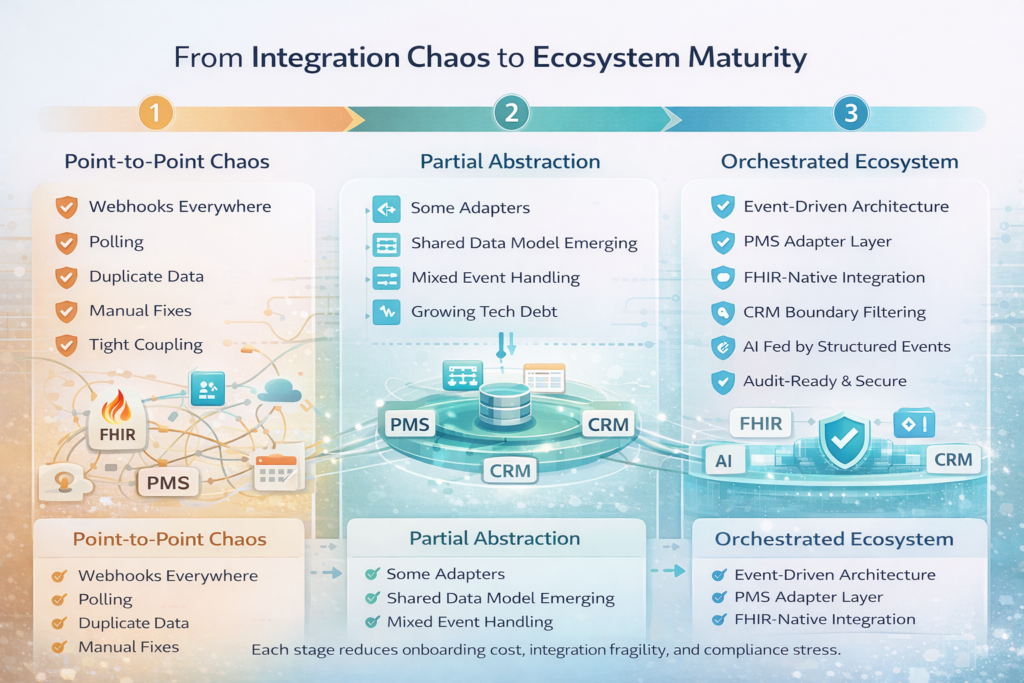
The Integration Maturity Path
Most telehealth platforms evolve through integration maturity stages. Early-stage platforms have point-to-point integrations built opportunistically. Growth-stage platforms begin abstracting common patterns but still carry significant integration debt. Mature platforms have coherent integration architectures that make adding new integrations faster and more reliable than the previous one.
The goal isn’t perfection — it’s compounding returns. Every architectural decision that increases integration coherence makes the next integration cheaper, the next enterprise customer easier to onboard, and the next compliance audit less stressful.
Start with the event orchestration layer, even before you have many integrations to orchestrate. Build integration abstraction early, before you have a dozen point-to-point connections to refactor. Establish API security standards before an enterprise customer’s procurement team asks for them.
The organizations that will lead telehealth in 2026 and beyond are building ecosystems today. The CTOs who understand that interoperability is a strategic capability — not just a technical checkbox — are the ones whose platforms will still be relevant when the next wave of healthcare technology arrives.